Download
1 / 1

E N D
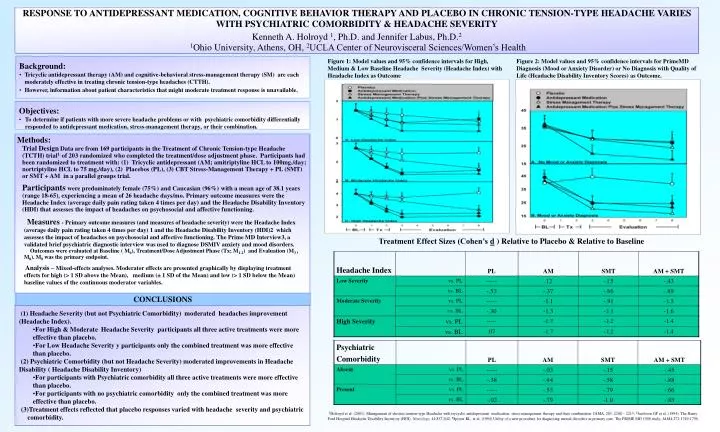
RESPONSE TO ANTIDEPRESSANT MEDICATION, COGNITIVE BEHAVIOR THERAPY AND PLACEBO IN CHRONIC TENSION-TYPE HEADACHE VARIES WITH PSYCHIATRIC COMORBIDITY & HEADACHE SEVERITYKenneth A. Holroyd 1, Ph.D. and Jennifer Labus, Ph.D.21Ohio University, Athens, OH, 2UCLA Center of Neurovisceral Sciences/Women’s Health • Background: • Tricyclic antidepressant therapy (AM) and cognitive-behavioral stress-management therapy (SM) are each moderately effective in treating chronic tension-type headaches (CTTH). • However, information about patient characteristics that might moderate treatment response is unavailable. Figure 1: Model values and 95% confidence intervals for High, Medium & Low Baseline Headache Severity (Headache Index) with Headache Index as Outcome Figure 2: Model values and 95% confidence intervals for PrimeMD Diagnosis (Mood or Anxiety Disorder) or No Diagnosis with Quality of Life (Headache Disability Inventory Scores) as Outcome. • Objectives: • To determine if patients with more severe headache problems or with psychiatric comorbidity differentially responded to antidepressant medication, stress-management therapy, or their combination. • Methods: • Trial DesignData are from 169 participants in the Treatment of Chronic Tension-type Headache (TCTH) trial1. of 203 randomized who completed the treatment/dose adjustment phase. Participants had been randomized to treatment with: (1) Tricyclic antidepressant (AM; amitriptyline HCL to 100mg./day; nortriptyline HCL to 75 mg./day), (2) Placebos (PL), (3) CBT Stress-Management Therapy + PL (SMT) or SMT + AM in a parallel groups trial. • Participants were predominately female (75%) and Caucasian (96%) with a mean age of 38.1 years (range 18-65), experiencing a mean of 26 headache days/mo. Primary outcome measures were the Headache Index (average daily pain rating taken 4 times per day) and the Headache Disability Inventory (HDI) that assesses the impact of headaches on psychosocial and affective functioning. • Measures - Primary outcome measures (and measures of headache severity) were the Headache Index (average daily pain rating taken 4 times per day) 1 and the Headache Disability Inventory (HDI)2 which assesses the impact of headaches on psychosocial and affective functioning.The Prime MD Interview3, a validated brief psychiatric diagnostic interview was used to diagnose DSMIV anxiety and mood disorders. • Outcomes were evaluated at Baseline ( M0), Treatment/Dose Adjustment Phase (Tx; M1-2) and Evaluation (M3 , M8). M8 was the primary endpoint. • Analysis – Mixed-effects analyses. Moderator effects are presented graphically by displaying treatment effects for high (> 1 SD above the Mean), medium (± 1 SD of the Mean) and low (> 1 SD below the Mean) baseline values of the continuous moderator variables. Treatment Effect Sizes (Cohen’s d ) Relative to Placebo & Relative to Baseline CONCLUSIONS • (1) Headache Severity (but not Psychiatric Comorbidity) moderated headaches improvement (Headache Index). • For High & Moderate Headache Severity participants all three active treatments were more effective than placebo. • For Low Headache Severity y participants only the combined treatment was more effective than placebo. • (2) Psychiatric Comorbidity (but not Headache Severity) moderated improvements in Headache Disability ( Headache Disability Inventory) • For participants with Psychiatric comorbidity all three active treatments were more effective than placebo. • For participants with no psychiatric comorbidity only the combined treatment was more effective than placebo. • (3)Treatment effects reflected that placebo responses varied with headache severity and psychiatric comorbidity. 1Holroyd et al. (2001). Management of chronic tension-type Headache with trycyclic antidepressant medication, stress management therapy and their combination. JAMA, 285, 2208 – 2215; 2Jacobson GP et al. (1994). The Henry Ford Hospital Headache Disability Inventory (HDI). Neurology, 44:837-842; 3Spitzer RL, et al. (1994) Utility of a new procedure for diagnosing mental disorders in primary care: The PRIME MD 1000 study. JAMA;272:1749-1756.