Download
1 / 2
20 likes | 160 Views
Intra-Operative Radiation Therapy for Treatment of Early Stage Breast Cancer: Short Term Results from a Single Institution Clinical Trial Using Electronic Brachytherapy with a Disposable Balloon Applicator

E N D
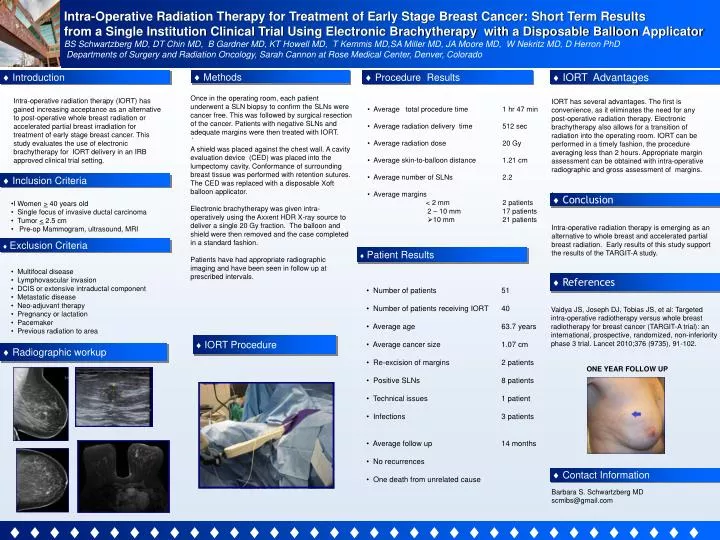
Intra-Operative Radiation Therapy for Treatment of Early Stage Breast Cancer: Short Term Results from a Single Institution Clinical Trial Using Electronic Brachytherapy with a Disposable Balloon Applicator BS Schwartzberg MD, DT Chin MD, B Gardner MD, KT Howell MD, T Kemmis MD,SA Miller MD, JA Moore MD, W Nekritz MD, D Herron PhD Departments of Surgery and Radiation Oncology, Sarah Cannon at Rose Medical Center, Denver, Colorado Logo Introduction Methods Procedure Results IORT Advantages Intra-operative radiation therapy (IORT) has gained increasing acceptance as an alternative to post-operative whole breast radiation or accelerated partial breast irradiation for treatment of early stage breast cancer. This study evaluates the use of electronic brachytherapy for IORT delivery in an IRB approved clinical trial setting. • Average total procedure time 1 hr 47 min • Average radiation delivery time 512 sec • Average radiation dose 20 Gy • Average skin-to-balloon distance 1.21 cm • Average number of SLNs 2.2 • Average margins • < 2 mm 2 patients • 2 – 10 mm 17 patients • 10 mm 21 patients • IORT has several advantages. The first is convenience, as it eliminates the need for any post-operative radiation therapy. Electronic brachytherapy also allows for a transition of radiation into the operating room. IORT can be performed in a timely fashion, the procedure averaging less than 2 hours. Appropriate margin assessment can be obtained with intra-operative radiographic and gross assessment of margins. • I Once in the operating room, each patient underwent a SLN biopsy to confirm the SLNs were cancer free. This was followed by surgical resection of the cancer. Patients with negative SLNs and adequate margins were then treated with IORT. A shield was placed against the chest wall. A cavity evaluation device (CED) was placed into the lumpectomy cavity. Conformance of surrounding breast tissue was performed with retention sutures. The CED was replaced with a disposable Xoft balloon applicator. Electronic brachytherapy was given intra-operatively using the Axxent HDR X-ray source to deliver a single 20 Gy fraction. The balloon and shield were then removed and the case completed in a standard fashion. Patients have had appropriate radiographic imaging and have been seen in follow up at prescribed intervals. . Inclusion Criteria Conclusion • I Women > 40 years old • Single focus of invasive ductal carcinoma • Tumor < 2.5 cm • Pre-op Mammogram, ultrasound, MRI • Multifocal disease • Lymphovascular invasion • DCIS or extensive intraductal component • Metastatic disease • Neo-adjuvant therapy • Pregnancy or lactation • Pacemaker • Previous radiation to area Intra-operative radiation therapy is emerging as an alternative to whole breast and accelerated partial breast radiation. Early results of this study support the results of the TARGIT-A study. • Controller Exclusion Criteria Patient Results References • Number of patients 51 • Number of patients receiving IORT 40 • Average age 63.7 years • Average cancer size 1.07 cm • Re-excision of margins 2 patients • Positive SLNs 8 patients • Technical issues 1 patient • Infections 3 patients • Average follow up 14 months • No recurrences • One death from unrelated cause Vaidya JS, Joseph DJ, Tobias JS, et al: Targeted intra-operative radiotherapy versus whole breast radiotherapy for breast cancer (TARGIT-A trial): an international, prospective, randomized, non-inferiority phase 3 trial. Lancet 2010;376 (9735), 91-102. ONE YEAR FOLLOW UP IORT Procedure Radiographic workup Contact Information Barbara S. Schwartzberg MD scmibs@gmail.com