Download
1 / 35
350 likes | 494 Views
Productivity Comparison CR vs. DR. The Economic Reason for CR & DR. CR Defined. CR Equipment. DR Defined. DR Equipment. Introduction. Workflow: CR-based Workflow: DR-based. Assumptions.

E N D
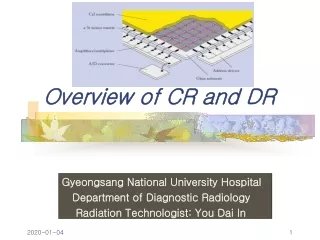
CR Defined CR Equipment
DR Defined DR Equipment
Introduction • Workflow: CR-based • Workflow: DR-based
Assumptions • The comparison will look at radiographic imaging, not the production of cross-sectional imaging on film, nor imaging for interventional radiology
Assumptions • CR and DR operation • An RIS and PACS are in place • The systems support DICOM MWL and PPS • Reading is done on PACS diagnostic workstations
Fundamental Steps in the Process • End the examination • Move the patient out of the examination room • Move images to the radiologist to be read
CR-based Workflow (Steps 1-2) • From the reception desk or inpatient schedule, determine the next patient to be examined • Call for the patient from the waiting room or floor
CR-based Workflow (Steps 3-4) • While the patient is changing or being put into the room, call up the worklist on the CR workstation • Select the appropriate patient and exam from the worklist
CR-based Workflow (Steps 5-8) • ID the plate • Position the patient and the CR plate • Set the generator and make the exposure • If there is more than one view, repeat the above three steps until done
CR-based Workflow (Steps 9-11) • Carry the CR plates to the plate reader • Stack the plates in the reader input • View the images on the CR reader workstation to be sure of correct position and exposure
CR-based Workflow (Steps 12-14) • If the images are not acceptable, return to re-take the necessary views • If the images are acceptable, check the patient ID and request number • If correct, send the study to PACS
CR-based Workflow (Steps 15-16) • If not correct, edit as needed, then send the study to PACS • Return to the exam room and have the patient dress or move to the holding area
CR-based Workflow • 16 steps • No film library steps • The major change is eliminating separate interaction with the RIS
CR-based Workflow: Variations • Some systems have the technologist select the patient and exam at the plate reader • Others use the ID and information recorded on the cassette to associate the images with the patient and exam • This changes where a step is done; it does not add a step
CR Alternatives • Dedicated chest and rapid-type rooms • Many CR Vendors are setting up relationships with DR vendors to meet this need
DR-based Workflow (Steps 1-3) • From the reception desk or inpatient schedule, determine the next patient to be examined • Call for the patient from the waiting room or floor • Have the patient change or moved into the exam room; log into the DR system
DR-based Workflow (Steps 4-7) • Select the patient and examination from the worklist • Position the patient • Set the generator and make the exposure • If more than one view is needed, repeat the above two steps
DR-based Workflow (Steps 8-11) • On the DR system or a QC workstation, view the images taken • If not acceptable (photon starvation/positioning), repeat the needed views • If acceptable, end the examination on the DR system • Discharge patient
DR-based Workflow • Reduced to 10 to 11 steps • No file room tasks • No interaction with cassettes
DR-based Workflow • A single system for capture, QC, and sending to PACS • Uses DICOM MWL and PPS to eliminate technologist interactions with the RIS • Eliminates carrying cassettes or plates • Eliminates a separate ID step
Additional Pros for DR Technology Direct capture means: • No phosphors • No scintillators • No intermediate steps • No light to diffuse or scatter • Nothing to degrade the quality of the digital signal
Downside of DR • Replace existing tables/wall Buckys • May have to replace the generator if the system cannot be integrated with it • Not having DICOM MWL and PPS obviates many of the advantages • Portable?
Find study to do Get patient Call up WL Pick from WL ID Plate Position patient Expose Add views? Carry plates Run plates View images Images OK? ID OK? Edit info Images to PACS DischargePt Schematic of Workflows Film-based CR-based DR-based Find study to do Find study to do Get paperwork Get patient Get patient Login to DR Begin exam RIS Pick from WL Position patient Expose Position patient Add views? Expose Flash ID Add views? Carry cassettes Process films Reload film Pick up films QC films View images Films OK? Images OK? Log exam in RIS Films to FL Locate master Discharge Pt End DR exam Make exam folder Log into RIS Discharge Pt Put in TBR slot Complete exam Load alternator Log exam Log loc in RIS
Other Workflow Considerations • Poor planning can defeat the advantages of CR and DR • If you design a department for technologist and patient movement as though you were using film, you may create problems
Planning Considerations • For CR, a rate-limiting step may be how far the plate readers are from the examination rooms • Technologist walking time may become significant
Planning Considerations • For DR, poor layout may make moving patients into and out of the rooms a rate-limiting step • Don’t just consider space when designing for film replacement; plan around “traffic flow” as well26
Additional Workflow • These workflow examples stop at the step at which the radiologist would interpret the exam • There are additional workflow improvements for PACS over film, but there is less of an impact from particular imaging methods
CR vs. DR • An objective assessment and comparison of computed radiography (CR) versus digital radiography (DR) and screen-film for performing upright chest examinations on outpatients is presented in terms of: • Workflow • Productivity • Speed of service • Potential cost justification
How Was The Study Conducted • Perceived ease of use and workflow of each device was collected via a technologist opinion survey. • Productivity is measured as the rate of patient throughput from normalized timing studies. • The overall speed of service is calculated from the time of examination ordering as stamped in the RIS, to the time of image availability on the PACS, to the time of interpretation rendered (from the Transcription System). • A cost comparison is discussed in terms of potential productivity gains and device expenditures. Comparative results of a screen-film (analog) dedicated chest unit versus a CR reader and a DR dedicated chest unit show a higher patient throughput for the digital systems.
The Statistics • A mean of 8.2 patients were moved through the analog chest room per hour, versus 9.2 patients per hour using the CR system and 10.7 patients per hour with the DR system. • This represents a 12% increase in patient throughput for CR over screen-film; • a 30% increase in patient throughput for DR over screen-film, which is statistically significant; and • a 16% increase in patient throughput for DR over CR, which is not statistically significant.
Measurements • Measured time to image availability for interpretation is much faster for both CR and DR versus screen-film: • With the mean minutes to image availability calculated as 29.2 ± 14.3 min for screen-film • 6.7 ± 1.5 min for CR • 5.7 ± 2.5 min for DR • This represents an improved time to image availability of: • 77% for CR over screen-film • 80% for DR over screen-film • 15% for DR over CR These results are statistically significant (P < .0001) for both CR over screen-film and DR over screen-film but not statistically significant for DR over CR.
Conclusion • A comparison of the digital technology costs illustrates that the high cost of DR may not be justifiable unless a facility has a steady high patient volume to run the device at or near 100% productivity. • Both CR and DR can improve workflow and productivity over analog screen-film in a PACS for delivery of projection radiography services in an outpatient environment. • Cost justification for DR over CR appears to be tied predominantly to high-patient volume and continuous rather than sporadic use patterns.
Additional Notes • There is a potential for workflow improvement in moving from film to CR and from CR to DR • These improvements require integration with HIS, RIS as well as the Transcription/Dictations Systems • Don’t forget department layout effects on workflow (location, location, location)