Download
1 / 58
600 likes | 847 Views
Adrenocorticosteroids and Adrenocortical Antagonists. Adrenal Gland. Adrenal cortex – mineralocorticoids, glucocorticoids, adrenal androgens (androstenedione and dehydroepiadrosterone) Adrenal medulla - catecholamines. Adrenal Cortex.

E N D
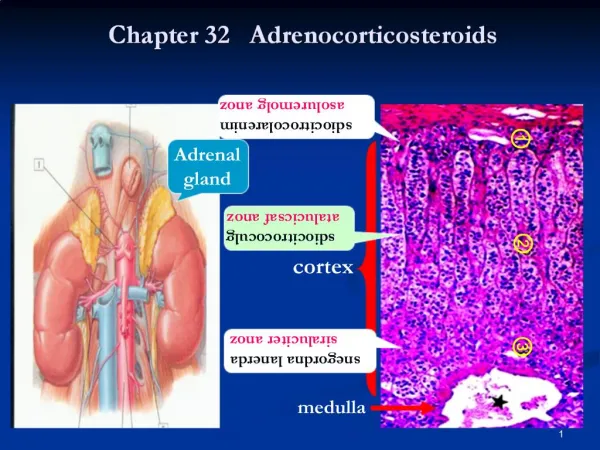
Adrenal Gland • Adrenal cortex – mineralocorticoids, glucocorticoids, adrenal androgens (androstenedione and dehydroepiadrosterone) • Adrenal medulla - catecholamines
Adrenal Cortex • Outer zone (zona glomerulosa) – secretes mineralocorticoids - receptors for angiotensin II and express aldosterone synthase; do not atrophy • Inner zone (zona fasciculata and reticularis) – secrete glucocorticoids and adrenal androgens - expresses 17α-hydroxylase and 11β-hydroxylase; results in atrophy
ACTH • a peptide of 39 amino acids • amino acids 15 – 18: high affinity binding • amino acids 6 – 10: receptor activation • synthesized from pro-opiomelanocortin (POMC)
ACTH • Stimulates the synthesis and release of adrenocortical hormones • Human ACTH – G-protein coupled receptor family → activates adenyl cyclase → ↑ intracellular cyclic AMP (2nd messenger for most steroidogenesis)
Regulation of ACTH secretion • Hypothalamic – Pituitary – Adrenal axis (HPA axis) - 3 levels of regulation: 1. diurnal rhythm in basal steroidogenesis 2. negative feedback regulation 3. marked increases in steroidogenesis in response to stress
Steroid hormone production • rate limiting step – conversion of cholesterol to pregnanolone • sources of cholesterol: circulating cholesterol (LDL), cholesterol esterase, de novo biosynthesis
Adrenal Cortex • Produce and releases natural adrenocortical hormones • Uses: a. diagnosis and treatment of disorders of adrenal function b. treatment of inflammatory and immunologic disorders
Adrenocorticosteroids Classification: A. Mineralocorticoids B. Glucocorticoids C. Gonadal Androgens
A. Glucocorticoids Naturally-occurring: Cortisol Kinetics: 10-20 mg daily; circadian rhythm; bound to CBG (90%), albumin (5%); t ½ =60-90 mins.; liver; 1/3 excreted as dihydroxyketone metabolites
B. Mineralocorticoids 1. Aldosterone – zona glomerulosa - promotes reabsorption of Na+ from the distal convoluted tubules and proximal collecting tubules; loosely coupled with K+ and H+ ions - secreted at a rate of 100-200ug/d; t ½ 15-20mins; excreted in the urine as tetrahydroaldosterone and 3-oxo-glucoronide
2. Deoxycortisone (DOC) – serves as precursor of aldosterone 3. Fludrocortisone – most widely used; both mineralocorticoid and glucocorticoid activity
C. Adrenal Androgens - dehydroepiandrosterone (DHEA) and androstenedione - they do not stimulate or support major androgen dependent pubertal changes in humans) - used in SLE and women with adrenal insufficiency
Dynamics: MOA: bind to cytosol receptors (steroid receptor complex) alters gene expression by binding to glucocorticoid-response element (GREs)
Physiologic effects Carbohydrate and protein metabolism: protect glucose-dependent tissues from starvation ( gluconeogenesis, glycogen synthesis) periphery: ↓glucose utilization, ↑protein breakdown (amino acids), activate lipolysis (glycerol) catabolic effects: decrease muscle mass, atrophy of lymphoid tissue, negative nitrogen balance, thinning of the skin
Physiologic effects (cont.): • Lipid metabolism: redistribution of body fat (buffalo hump, moon facies, supraclavicular area with loss of fat in the extremities) induce lipolysis in adipocytes ( FFA) • Electrolyte and water balance: enhances the reabsorption of Na (aldosterone) renal excretion of free water and interferes with Ca uptake, while there is ↑Ca excretion by the kidneys (glucocorticoids)
Physiologic effects (cont.) • Cardiovascular system: - mineralocorticoid-induced changes – hpn - enhance vascular reactivity to other vasoactive substances • Skeletal muscle: normal function (steroid myopathy) • CNS: neurosteroids (regulate neuronal excitability)
Physiologic effects: • Formed elements of blood: minor effects on hgb and erythrocyte production; affect circulating WBC (Addison’s: lymphocytosis, ↑ mass of lymphoid tissue) • Anti-inflammatory and Immunosuppressive action • alter immune response of lymphocytes - ↓release of vasoactive and chemoattractive factors, - diminished secretion of lipolytic and proteolytic enzymes - decreased extravasation of leukocytes to injury - decreased fibrosis - effect on cytokine production
Other effects: ↑amounts – insomnia, euphoria, depression, pseudomotor cerebri ↓amounts – psychiatric depression large doses – peptic ulcer, promote fat distribution; vit D antagonist on Ca absorption; ↑ # of platelets and RBCs absence – impaired renal function fetal lung effects
Classification of Adrenocorticosteroids I. Short to medium-acting glucocorticoids: a. Hydrocortisone (cortisol) b. Cortisone c. Prednisone d. Prednisolone e. Methylprednisolone f. Meprednisone
II. Intermediate-acting glucocorticoids a. Triamcinolone b. Paramethasone c. Fluprednisolone III. Long-acting glucocorticoids a. Betamethasone b. Dexamathasone IV. Mineralocorticoids a. Fludrocortisone b. desoxycorticosterone acetate
Therapeutic principles • Dose selection by trial & error; Needs frequent evaluation • Single dose: No harm • Few days therapy unlikely to be harmful • Incidence of side effects related to duration of therapy • Use is only palliative (except replacement therapy) • Inter-current illness: Dose is doubled • Abrupt cessation of prolonged high dose leads to adrenal insufficiency (contraindicated)
Addison described : . general languor and debility . remarkable feebleness of the heart's action . irritability of the stomach . peculiar change of the color of the skin
Synthetic Steroids Kinetics: source – cholic acid (cattle) or steroid sapogenins (diosgenin, hecopenin); absorption: oral, IV, IM, sites of local administration prolonged effects: occlusive dressing, large areas – may cause suppression of HPA axis
Kinetics (cont.) • Transport: 90% bound to CBG (transcortin – high affinity but low total binding capacity) and albumin (low affinity but high binding capacity) 10% unbound • Metabolism –liver • Excretion - kidneys
Therapeutic Uses: A. Replacement Therapy 1. Adrenal Insufficiency a. Acute adrenal insufficiency ssx: GIT symptoms, dhn, hypoNa, hyperK, weakness, lethargy, hypotension cause: disorder of the adrenal abrupt withdrawal of glucocorticoids at high doses or prolonged use mgt: IV : D5 0.3%NaCl solution Monitor for fluid overload Hydrocortisone (cortisol) 100mg bolus, ffed by 100mg every 8 hrs. ; once stable, may give 25mg IM hydrocortisone every 6-8hrs.; thereafter, same mgt with chronic adrenal insufficiency
1. Adrenal Insufficiency (cont.) b. Chronic Adrenal Insufficiency (Addison’s disease) ssx:hyperpigmentation, wt. loss, inability to maintain fasting blood sugar, weakness, fatigue, hypotension cause: primary adrenal insufficiency, tuberculosis mgt: Hydrocortisone 20-30mg/day BID Fludrocortisone acetate 0.05 – 0.2mg/day (valuable indicator of adequate replacement: disappearance of hyperpigmentation and resolution of electrolyte abnormalities) -monitor plasma ACTH levels or measure urinary free cortisol; dosage adjustments for stress
Therapeutic Uses (cont.)2. Adrenocortical hypo- and hyperfunctioning a. Congenital Adrenal Hyperplasia ssx: after puberty with infertility, hirsutism, amenorrhea and acne; female pseudohermaphroditism; accelerated linear growth but height at maturity is reduced; salt wasters – CV collapse (volume depletion) cause: Genetic disorder; activity of enzymes required for the biosynthesis of corticosteroid is deficient (21 β hydroxylase) mgt: 1st seen as acute adrenal crisis oral hydrocortisone 0.6mg/kg/day BID or TID fludrocortisone acetate 0.05-0.2mg/day treatment in-utero: mothers at risk – glucocorticoid therapy is initiated before 10 weeks gestation ffed by genotyping and sex determination
b. Cushing’s syndrome cause: pituitary adenoma, tumors of the adrenal gland ssx: round, phletoric face, truncal obesity, muscle wasting, thinning, purple striae and easy bruising of the skin, poor wound healing, osteoporosis mgt: surgery hydrocortisone 300 mg IV on the day of the surgery, then maintenance oral dose
B. Stimulation of fetal lung maturation –betamethasone 12mg ffed by 12mg 18-24 hrs. later C.Nonendocrine Diseases 1. Rheumatic disorders – suppress the disease and minimize resultant tissue damage mgt: prednisone 10 mg/kg/day (taper thereafter by decreasing 1mg/kg/day every 2-3 wks) intraarticular injection: triamcinolone acetonide osteoarthritis : intraarticular injections with interval of 2-3 mos. to minimize complications
C. Non-Endocrine Diseases (cont.) 2. Renal Disorders – nephrotic syndrome mgt: prednisone: 1-2 mg/kg x 6 wks, ffed. by gradual tapering over 6-8 wks or alternate-day therapy (diminished proteinuria in 85% pts in 2-3 wks and 95% pts will have remission in 3 mos. - membranous glomerulonephritis mgt: alternate-day prednisone 8-10 wks ffed by 1-2 month period of tapering
C. Non-Endocrine Diseases (cont.) 3. Allergic Disease – epinephrine 0.5ml of a 1:1000 solution IM or SQ, repeated every 15 mins up to 3 doses is needed (anaphylaxis) - onset of action of glucocorticoid is delayed
C. Non-Endocrine Diseases (cont.) 4. Bronchial Asthma – role of inflammation in the immunopathogenesis - onset of action is delayed for 6 – 12 hrs. mgt: IV methylprednisolone 60-120mg initially ffed. by oral prednisone 40-60mg daily as the attack resolves inhaled steroids – reduces bronchial hyperreactivity with les suppression of adrenal function (dysphonia or oropharyngeal candidiasis)
C. Non-Endocrine Diseases (cont.) 5. Infectious Disease – P. carinii pneumonia – increases oxygenation and decreases the incidence of respiratory failure and mortality H. influenzae type b meningitis – decrease the long-term neurological impairment 6. Ocular disease – 0.1% dexamethasone - C/I: herpes simplex keratitis (clouding of the cornea) , glaucoma
C. Non-Endocrine Diseases (cont.) 7. Skin diseases – inflammatory dermatoses 8. GIT diseases – inflammatory bowel disease 9. Hepatic diseases – prednisolone – 80% histologic remission in pts. with chronic, active hepatitis 10. Malignancies – ALL, lymphomas 11. Cerebral edema 12. Miscellaneous dis – Sarcoidosis (induce remission), thrombocytopenia (decrease bleeding tendency), organ transplantation, spinal cod injury