Download
1 / 43
430 likes | 576 Views
Mechanisms of Injury and Repair. Classification of injury. The repair process. Ligament healing. Functional knee brace. Classifications of injury. According to mechanism: primary vs secondary. According to tissues: soft tissues vs hard tissues. (Oakes 1992). Primary injuries (1).

E N D
Mechanisms of Injury and Repair Classification of injury. The repair process. Ligament healing. Functional knee brace.
Classifications of injury • According to mechanism: • primary vs secondary. • According to tissues: • soft tissues vs hard tissues. (Oakes 1992)
Primary injuries (1) • direct/extrinsic: usually high forces, result in severe injuries. • indirect/intrinsic: eccentric overload of musculotendinous units.
Primary injuries (2) • Overuse injury: repetitive friction leads to tenosynovitis. • Chronic repetitive microfatigue: stress # or Osgood-Schlatter’s disease.
Secondary injuries • Short term: previous mismanaged injury e.g. resolving phase of inflammation when pain is down. • Long term: e.g. secondary O.A. knee due to ACLD.
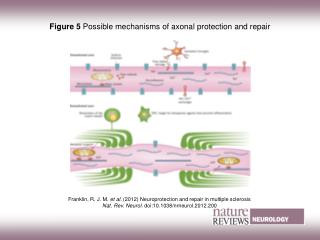
The repair process (1) • Three phases of tissue repair in general. • Inflammation phase. • Repair phase. • Remodelling phase.
The repair process (2) • Acute inflammation at initial 72 hours. • New blood vessels to the wound. • Healing: wound must be clean and blood must be available. • Little inflammation, healing is slow; excessive inflammation, over scarring.
The repair process (3) • Matrix and cellular proliferation phase 72 hours to 6 weeks. • Active synthesis of collagen/proteoglycan matrix forming granulation tissue. • Induce epithelialization and wound contraction. • Neovascularization probably controlled by growth factors.
The repair process (4) • New collagen is mainly type III. • Collagen fibrils are small and not oriented. • Poor material properties of the scar tissue. • Remodelling and maturation: 6 weeks to several months. • Loading, movements determine collagen maturation and alignment.
Ligament healing 1 • Proximity of rupture ends. • Availability of repair cells. • Synovial fluid (the hostile environment). • Load during remodelling.
Ligament healing 2 • Complete sectioning of the PLB of goat ACL (Ng et al 1996 AJSM). • No surgical repair. • Free activities in a farm.
Ligament healing 3 • Mechanical testing at 12 wk (n=3), 24 wk (N=3), 52 wk (N=3) and 3 yr (N=2). • Laxity testing. • Instron material testing for UTS, stiffness, Young’s modulus and load relaxation.
Ligament healing 4 • Evidence of healing at 12 weeks with translucent fibrous tissue. • Repair tissues appeared normal at 1 year. • Indistinguishable repair tissue from normal tissue surrounding the repair at 3 years. • The whole ligament bundle has grown in size.
Ligament healing 5 • No significant difference in laxity among all groups. • The intact amb provided the restrain? • Not enough drawer force to test the ligament?
Ligament healing 6 • General increase in normalised UTS with time. • Significantly higher UTS at 3 years than 12 weeks. • Control UTS: 1167 N; UTS 3 years: 1493N • Ligament failure at 12 and 24 weeks, but bony avulsion at 3 years.
Ligament healing 7 • General increase in stiffness with time. • Significantly higher stiffness at 3 years than 12 weeks. • Control stiffness: 258 N/mm; 12 weeks: 146 N/mm; 1 year: 198 N/mm; 3 years: 250 N/mm.
Ligament healing 8 • General increase in Young’s modulus with time. • Control modulus: 487 MPa; 12 weeks: 257 MPa; 1 year: 408 MPa; 3 year: 351 MPa. • Why is stiffness different from Young’s modulus? • Clinical implication.
Ligament healing 9 • No general trend in load relaxation pattern with time. • Frank (1985) found scar would load relax quicker than normal tissues. • This could result in overloading to the secondary restraints.
Functional knee brace (1) • Three functions: biomechanical physiological proprioceptive
Functional knee brace (2) • Little mechanical protection (Bagger, 1992; Beynnon, 1992; Warming & Jorgensen, 1998). • Increase energy consumption (Highgenboten, 1991). • increasing relaxation pressure of muscles (Styf, 1994).
Functional knee brace (3) • Improve proprioception and AP body sway (Kuster, 1999). • Improve cutaneous sensation (Beynnon, 1999; Birmingham, 1998). • Controversies among studies on knee brace. • Mechanical vs. non-mechanical components of the braces. • Tests to simulate sports activities.
Study objectives (Wu, Ng, Mak 2001a & b) • To compare: (1) no brace, (2) Donjoy legend functional brace, (3) mechanical placebo brace.
Parameters measured • Running and turning. • Jumping and landing. • Isokinetic performance. • Joint sense.
Methods • Subjects • 31 subjects aged 15-40 with single limb injury. • Arthroscopic ACL reconstruction with semitendinosus by the same surgeon. • At least 5 months post-operation.
Running and Turning Test • Subjects ran on a “figure-of-eight” runway of 22 m long for 10 laps. • Time of running and turning on each side recorded.
Jumping and landing Test • Subject ran on a semicircular path. • Jumped and turned internally with the affected leg. • Landed on a floor marker (20Cm X 28Cm). • Accuracy of landing and time to complete the run/jump task recorded.
Isokinetic Test • 60o/s & 180o/s. • 0 - 60o of knee flexion. • Peak torque and total work recorded.
Copying of knee joint angle • Five pre-set angles by passive positioning. • Subjects indicated the perceived angle on a knee model (Attfield et al 1996). • Mean Difference in the angles recorded.
Conclusion 1 • Subjects ran 3.2 % - 4.6 % slower in both bracing conditions than no brace. • Similar to the report of increase energy expenditure values (Highgenboten 1991).
Conclusion 2 • Bracing enhanced the static knee joint sense. • Improvement was not due to mechanical restraint of the brace.
Conclusion 3 • Bracing had slowed down running/turning. • Bracing did not improve isokinetic and jumping performance.