Download
1 / 111
1.11k likes | 1.13k Views
Learn about the symptoms, progression, and treatment options for alcohol intoxication and withdrawal. Understand the risks, effects, and best practices for managing these conditions effectively.

E N D
Alcohol and Sedative Hypnotics Ellen A. Ovson, M.D., F.A.S.A.M. Medical Director Bradford Health Services, Madison, Alabama
“If the patient be in the prime of life and if from drinking he has trembling hands, it may be well to announce beforehand either delirium or convulsions” • Hippocrates circa 400 BC
Intoxication • BAC 20 mg% to 99 mg% • Loss of muscular coordination • Changes in mood, personality, and behavior
Intoxication • BAC 100 mg% to 199 mg% • Neurologic impairment • Prolonged reaction time • Ataxia • Incoordination • Mental impairment
Intoxication • BAC 200 mg% to 299 mg% • Marked ataxia • Nausea and vomiting
Intoxication • BAC 300 mg% to 399 mg% • Hypothermia • Severe dysarthria • Amnesia • Stage I anesthesia
Intoxication • BAC 400 mg% to 799 mg% • Alcoholic coma • Progressive obtundation • Decreased respiration • Decreased blood pressure • Decreased body temperature • Urinary incontinence or retention • Reflexes markedly decreased or absent
Intoxication • BAC 600 mg% to 800 mg% • Often fatal • Death may occur from loss of airway protective reflexes (obstruction from flaccid tongue) • Pulmonary aspiration of gastric contents • Profound CNS depression
Management of Intoxication • Supportive • Primary goals • Prevent respiratiory depression • Protect airway (prevent aspiration) • Survival is probable with respiratory and cardiovascular support • IV glucose and thiamine (alcohol impairs glucogenesis)
Management of Intoxication • Emesis / gastric lavage not indicated (EtOH rapidly absorbed) • Charcoal does not absorb alcohol • Enhancement of elimination has no role • Hemodialysis is effective, but rarely indicated since treatment is supportive only • No effective antagonist (flumazenil not effective) • Agitation best managed non-pharmacologically
Management of Intoxication • Rate of metabolism follows zero order kinetics • Independent of time and concentration of the drug • Elimination occurs at a rate of 15 to 20 mg/dl/hr
Alcohol Withdrawal • Begins 6 to 24 hrs after last drink • Onset sometimes before BAC reaches 0 • Early symptoms include anxiety, sleep disturbance, vivid dreams, anorexia, nausea, and headache • Physical signs include tachycardia, elevation of blood pressure, hyperactive reflexes, sweating, and hyperthermia • Tremor of hands/or tongue, 6 to 8 cycles/sec (exaggeration of normal physiologic tremor on EMG)
Alcohol Withdrawal • Seizures may occur, typically within 48 hrs • Delirium tremens may begin 48 to 72 hrs after last drink, preceded by symptoms of early withdrawal • Profound sympathetic hyperactivity (tachycardia, hypertension, fever, diaphoresis) • Mortality rate 1% to 5%, increases with delayed diagnosis, inadequate treatment, and concurrent medical illness
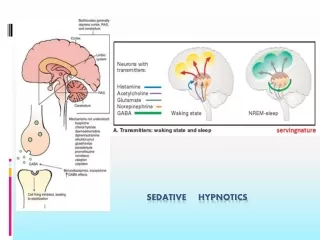
Alcohol Withdrawal • Effect of alcohol exerted through GABA • Sedation, muscle relaxation, increased seizure threshold • Chronic alcohol exposure leads to adaptive suppression of GABA activity • Abstinence produces sudden relative deficiency in GABA activity resulting in anxiety, increased psychomotor activity, and predisposition to seizures
Alcohol Withdrawal • Alcohol inhibits sensitivity to autonomic adrenergic systems • Chronic alcohol uptake results in upregulation • Discontinuation of alcohol results in rebound overactivity of central and peripheral noradrenergic systems • Increased sympathetic autonomic activity from the locus ceruleus contributes to tachycardia, hypertension, tremor, diaphoresis, and anxiety
Withdrawal Hallucinations • In mild withdrawal, may experience perceptual distortions of visual, auditory, or tactile nature (too bright, too loud, pins and needles) • Frank hallucinations may develop in severe withdrawal
Withdrawal Hallucinations • Visual hallucinations are most common and frequently involve animals • Auditory hallucinations begin as unformed sounds (clicks or buzzing) and may progress to voices • Often friends and relatives, often accusatory • Tactile hallucinations may involve bugs crawling on the skin
Withdrawal Hallucinations • In milder cases of withdrawal, the patient’s sensorium is otherwise clear and the patient retains insight that the hallucinations are not real • In more severe withdrawal, this insight may be lost
Withdrawal Seizures • Generalized major motor seizures • May occur singly or in a burst of several seizures over a few hours • Onset is usually 8 to 24 hours after last drink and may occur before BAC zero • Fewer than 3% progress to status epilepticus (but alcohol involved in 25% of status epilepticus)
Withdrawal Seizures • Seizures peak 24 hours after last drink, corresponding with EEG abnormalities (increased amplitude, photomyoclonic response, and spontaneous paroxysmal activity) • EEG changes transient
Withdrawal Seizures • Risk of seizures appears to be genetically influenced • Increased risk in those with prior history of withdrawal seizures • Increased risk in those undergoing concurrent sedative-hypnotic withdrawal
Withdrawal Seizures • Kindling effect • Increased risk of seizures as an individual undergoes repeated withdrawals
Alcohol Withdrawal Delirium • Delirium tremens generally appears 72 to 96 hours after last drink
Alcohol Withdrawal Delirium • Marked tachycardia, tremor, diaphoresis, fever
Alcohol Withdrawal Delirium • Global confusion; disorientation to place and time; may become absorbed in a separate psychic reality • Hallucinations frequent, may have no insight, and therefore may be very frightening
Alcohol Withdrawal Delirium • Marked psychomotor activity may develop • Severe agitation in some cases • Persistent low level motor activity in others • Severe disruption in sleep-wake cycle is common; absence of clear sleep for days
Alcohol Withdrawal Delirium • Duration is variable, 2 to 3 days in most studies • May last few hours • May last several days (report of confusion lasting 50 days before clearing)
Alcohol Withdrawal Delirium • Amount of daily intake and duration of heavy drinking have not been correlated consistently to the risk of severe withdrawal
Alcohol Withdrawal Delirium • BAC >300 mg% on presentation at higher risk of DT’s • Withdrawal seizure at presentation increases risk of DT’s • Older patients at higher risk of confusion and delirium, may not involve severe autonomic manifestations of classic DT’s
Alcohol Withdrawal Severity Scales • CIWA, and shortened version CIWA-Ar are most extensively studied • Documented reliability, reproducibility, and validity • <9 indicates mild withdrawal, 10 to 18 indicates moderate withdrawal, and >18 suggests severe withdrawal • High scores are predictive of seizures and delirium
Pharmacologic Management • ASAM Clinical Practice Guidelines (1997) reviewed literature on pharmacologic management of withdrawal • Evidence indicated that the cornerstone of pharmacologic management of withdrawal is the use of benzodiazepines
Benzodiazepines • Pharmacologically cross tolerant with alcohol • Produce the similar effect of enhancing GABA-induced sedation • Administration of benzodiazepines alleviates the acute deficiency of GABA activity that occurs with sudden cessation of alcohol
Benzodiazepines • All are similarly efficatious in reducing signs and symptoms of withdrawal
Benzodiazepines • Longer acting agents (diazepam and chlordiazepoxide) may be more effective in preventing seizures • Longer acting agents may provide a smoother withdrawal course • Longer acting agents may pose a risk for oversedation in the elderly and those with liver disease (shorter acting agents, lorazepam or oxazepam may be preferable).
Benzodiazepines • Rapid acting agents (diazepam, lorazepam, and alprazolam) offer more prompt control of symptoms • Rapid acting agents demonstrate greater abuse potential
Non-benzodiazepine sedative-hypnotics • Not as extensively studied • Size of studies not adequate to draw conclusions regarding efficacy in reduction of seizures and delirium • Benzodiazepines offer greater margin of safety with lower risk of respiratory depression as well as overall lower risk of abuse
Non-benzodiazepine sedative-hypnotics • “Phenobarbital, a long acting barbiturate, still is used by some programs, as it is long-acting, has well-documented anticonvulsant activity, is inexpensive, and has low abuse potential.”
Dose Determination • Fixed Schedule • Medication administered in fixed amounts at scheduled times for five to seven days • However, many patients can go through withdrawal with only minor symptoms and need little or no medication
Dose Determination • Symptom-triggered therapy • Patient is monitored with structured assessment scale and given medication only when symptoms cross a threshold of severity • Studies demonstrate as effective as fixed-dose regimen, but significantly less medication used and significantly shorter duration of detox • Facilitates delivery of large amounts of medication to patients with rapidly escalating symptoms, thus reducing undertreatment with fixed-dose schedule
Dose Determination • In certain patients, such as those with severe coronary artery disease, fixed-dose may be used to prevent development of even minor withdrawal symptoms • In patients with a history of alcohol withdrawal seizures, fixed-dose may be used since seizures usually occur early in the course of withdrawal
Dose Determination • Any detox regimen should allow for individualization with a mechanism to provide for large amounts of medication rapidly if needed.
Dose Determination • Benzodiazepines should be administered orally or intravenously • Lorazepam provides good intramuscular and sublingual absorption
Other Agents • Beta blockers and alpha adrenergic agonists are effective in ameliorating symptoms by reducing autonomic manifestations of withdrawal • No demonstrated efficacy in reducing seizures or delirium • Delirium is a rare side effect of beta blockers • Reduction in autonomic symptoms may mask progression of withdrawal and hinder reliability of withdrawal scales
Other Agents • Carbamazepine used in Europe for alcohol withdrawal • Equal efficacy to benzos for patients with mild to moderate withdrawal • Without toxicity over 7 day course of tx, less psychiatric distress, faster return to work, no impairment of learning, no abuse potential • Prevents withdrawal seizure in animal studies • Studies of adequate size to demonstrate efficacy in preventing withdrawal seizures or delirium not yet available
Other Agents • Antipsychotics are less effective than benzodiazepines to prevent delirium • Actually lead to increase rate of seizure • Widely used for agitation in withdrawal • Should never be used except in conjunction with benzodiazepines
Other Agents • Magnesium generally normal at onset of withdrawal, drops as withdrawal progresses, normalizes as symptoms subside • Only one randomized trial of magnesium during alcohol withdrawal documented • No difference in severity of withdrawal or rate of seizures, regardless of magnesium correction • Oral magnesium supplementation is without risk • Routine magnesium administration no longer recommended
Other Agents • Alcohol • No controlled trials comparing ethyl alcohol to benzos or placebo • IV administration requires very close monitoring • Numerous adverse effects • Use is discouraged by addiction specialists
Other Agents • Phenytoin • Recent studies failed to demonstrate efficacy of preventing recurrent withdrawal seizures • Benzos are extremely effective in preventing withdrawal seizures, and the addition of phenytoin does not lead to improved outcomes • Use of phenytoin in withdrawal has been largely abandoned
Other Agents • Thiamine • Thiamine deficiency may lead to Wernicke’s disease and the Wernicke-Korsakoff syndrome