Download
1 / 6
70 likes | 366 Views
In-hospital course of stroke patients with vs without AF. With AF. Without AF. More severe stroke on admission • Lower Barthel Index • Higher proportion with Rankin Scale score (%)

E N D
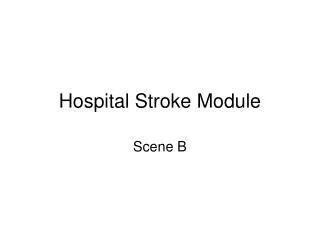
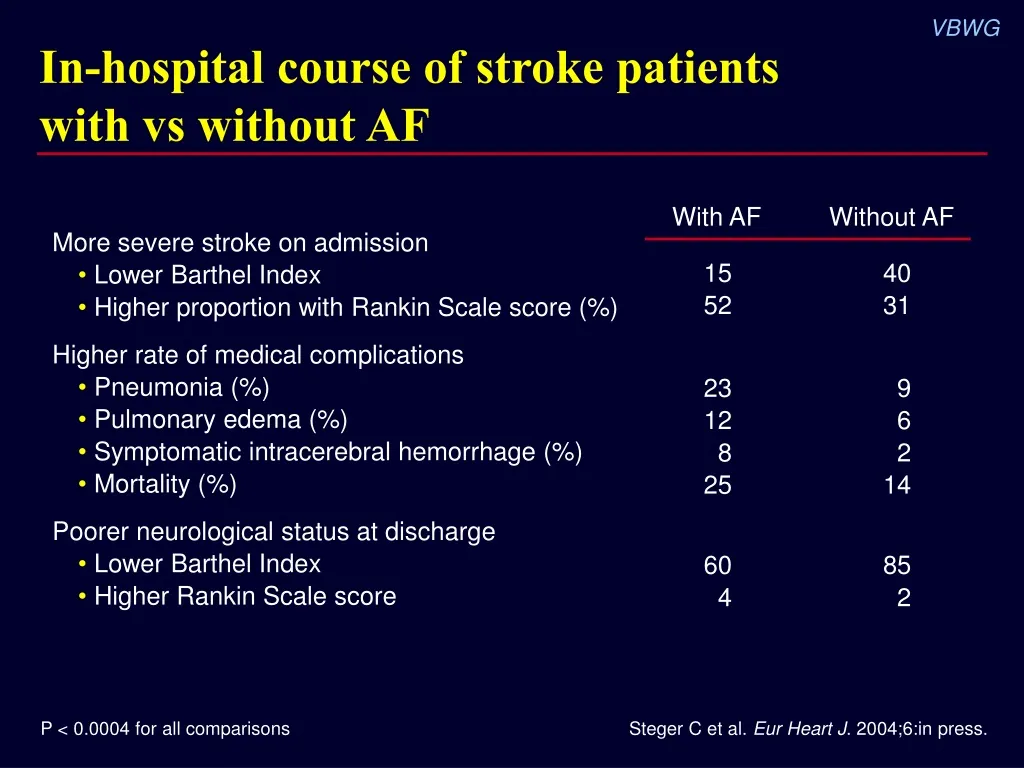
In-hospital course of stroke patients with vs without AF With AF Without AF More severe stroke on admission• Lower Barthel Index• Higher proportion with Rankin Scale score (%) Higher rate of medical complications• Pneumonia (%)• Pulmonary edema (%)• Symptomatic intracerebral hemorrhage (%)• Mortality (%) Poorer neurological status at discharge• Lower Barthel Index• Higher Rankin Scale score 1552 4031 2312825 96214 604 852 P < 0.0004 for all comparisons Steger C et al. Eur Heart J. 2004;6:in press.
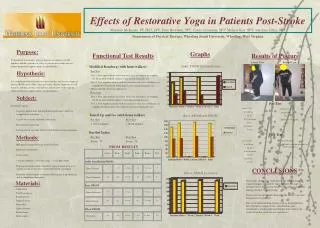
AF? AF? Detection of AF after acute stroke/TIA N = 149 Stroke/TIA No. AF detected Yes ECG AF? 4 (2.7%) No Additional ECG n = 145 Yes 6 (4.1%) No n = 139 24-hr Holter Yes 7 (4.9%) No 7-day ELR n = 88/132 Yes AF? 5 (5.7%) ELR = 2-lead event-loop recording device Jabaudon D et al. Stroke. 2004;35:1647-51.
ECG Holter ELR AFrisk(%) Monitoring time (hours) Risk of AF by duration of heart rhythm Jabaudon D et al. Stroke. 2004;35:1647-51.
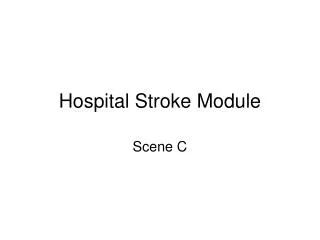
Recurrence of AF 13 months post-stroke/TIA 60 50 40 AFrecurrence(%) 30 20 10 0 ECG or 24-hr Holter 7-day ELR ELR = 2-lead event-loop recording device Jabaudon D et al. Stroke. 2004;35:1647-51.
Clinical challenge: Addressing the rising burden of AF and stroke • AF continues to present an enormous public health problem – Men and women >40 yrs have lifetime risk for AF of ~1 in 4 – Estimated 2.2 million Americans – May account for up to 140,000 strokes yearly • ECG and 24-hr Holter monitoring do not identify all stroke/TIA patients with AF • Many AF patients are not receiving anticoagulant therapy to prevent recurrent stroke Lloyd-Jones DM et al. Circulation. 2004;110:1042-6. AHA. Heart Disease and Stroke Statistics—2004 Update. Jabaudon D et al. Stroke. 2004;35:1647-51.
Role of anticoagulant therapy in secondary prevention of stroke • AF should be strongly suspected in all patients with acute stroke/TIA or TIA – All stroke/TIA patients with confirmed AF should receive anticoagulant therapy • Warfarin – Pro: Proven effective – Con: Need for frequent (and costly) monitoring and dose adjustment • New anticoagulants that offer fixed dosing with no monitoring are under investigation and may address warfarin’s shortcomings – Oral (direct thrombin inhibitors, ie, ximelagatran) – Parenteral (low–molecular-weight heparins, factor Xa inhibitors)