Download
1 / 12
120 likes | 227 Views
The Need for Quality Improvement : Challenges and Options. Indira Narayanan, MD Consultant MCHIP. Two Golden Truths. Mere PRESENCE of skilled birth attendants does not guarantee quality newborn care

E N D
The Need for Quality Improvement : Challenges and Options Indira Narayanan, MD Consultant MCHIP
Two Golden Truths • Mere PRESENCE of skilled birth attendants does not guarantee quality newborn care • Mere TRAINING of skilled birth attendants (even if competency based) does not guarantee quality newborn care 2
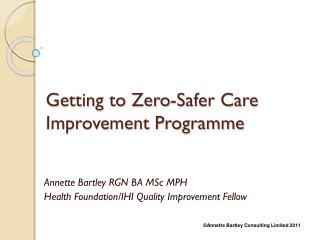
EVOLUTION OF SKILLS OF PROVIDERS IN 10 HZ(DRC) (At end of training all providers scored at least 80% ( most near 100%) when evaluated with checklists)
Providers who gained skills through interactionwith trained health workers gained similar competence
Supervision is not always in the job description of hospital staff Self learning and mentoring cultures limited Supervisors are in govt. offices - limited clinical skills, poor motivation for visits to peripheral centers – want incentives Supervision often considered long after training Peripheral centers are scattered and not sufficiently staffed Clinical competence needs support of commodities +referral system – inadequate cases necessitates more mannequins Some NB indicators are not in HMIS –therefore not collected Baseline / end-line surveys are costly Maintaining and improving quality of care through supervision: Challenges 23
Possible options to improve quality: Before training • Policies • Follow HBB guidelines for adapting • Advocate early for key indicators to be in HMIS –can serve as benchmarks for assessing quality of care /results • Drying/stimulation/warmth – regular part of ENC • Airway Clearing • Ventilation • Outcome • Plan for having key Information in delivery registers – case sheets/partographs more likely to be lost/ misplaced
Possible options to improve quality • Before Training (Cont’d) • Develop consensus on major issues with existing programs • Plan/get in place • Equipment, supplies and mannequins. Allow time for procurement in planning program activities • Resources for M & E – commence with additional columns/note books - plan use of benchmarks • During training course • Use terminologies that are widely understood in the country including peripheral health workers • Brainstorm+ develop plans for quality+ M & E • Brainstorm on how to get help for resuscitation
Possible options to improve quality During and after training • During training and evaluation including in OSCE 2 • Monitor method of placement of mask to get a better seal • Monitor (a) the health worker looks for appropriate chest expansion and (b) the facilitator verifies expansion • After training, while individual assessment through visits is ideal, it is time consuming and does not permit many workers to be covered, especially in peripheral centers. Additional methods of supervision include • Internalsupervision for larger centers/hospitals • Groupsupervision for health centers with few staff. • Explore innovative methods such as use for m Health for both M & E and quality of care
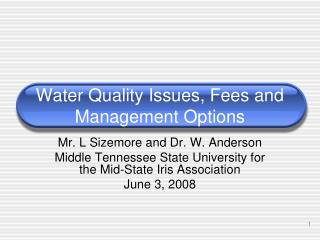
Late acquisition of equipment and insufficient number of cases may have resulted in decrease in competence at the first supervisory visit –improved with further support Group supervision: more workers are targeted (5 S1 compared to 12 S2 and 13 S3) – USAID/BASICS) Skills of Betioky (Madagascar) health workers on resuscitation techniques Percentage of average scores Follow-up 1 (N=5) Dec 08 Follow-up 2 (N:12) Feb 08 Follow-up 3 (N:13) Mar 08
Group supervision (modified collaborative approach): Advantages More agents are covered in a shorter time Agents help and motivate each other Fruitful exchanges on problems encountered in practice and possible solutions Opportunity for supervisors to provide suggestions for improvement to the group Easier to take decisions, define priorities, try solutions (PDSA) Useful for reviewing skills relating to cases that are infrequent such’ birth asphyxia’ or an sick newborn in health centers) Rotating sites can be useful to inspect other centers Facilitation by NGO’s helpful 24
Two Golden Rules Training alone not enough. We must consider : • Capacity building for • provision of documented good quality HBB care • Definition and documentation of the results
THANK YOU! www.mchip.net