Download
1 / 17
170 likes | 484 Views
GI7. CASE REPORT OF PERITONEAL TUBERCULOSIS. SALHI.K 1 ; AYAT.A 1 ;HELLARA.A 1 ;JERBI.S 2 ;MAHJOUB.B 1 ;BOUSSOFFARA.R 1 ; HAMZA.AH 2 ; SOUA.H; MT.SFAR 1 . 1 Service de Pediatrie CHU Taher Sfar Mahdia 2 Service de Radiologie CHU Taher Sfar Mahdia. INTRODUCTION:.

E N D
GI7 CASE REPORT OF PERITONEAL TUBERCULOSIS SALHI.K1; AYAT.A1 ;HELLARA.A 1;JERBI.S2 ;MAHJOUB.B1;BOUSSOFFARA.R1; HAMZA.AH2; SOUA.H; MT.SFAR1.1 Service de Pediatrie CHU TaherSfar Mahdia 2 Service de Radiologie CHU TaherSfar Mahdia
INTRODUCTION: • The peritoneum is one of the locations outside the most common pulmonary tuberculosis. • Peritoneal tuberculosis poses a public health problem in endemic regions of the world . • The diagnosis is difficult and still remains a challenge : insidious nature , variability of presentation and limitations of available diagnostic tests. • We report a case of an adolescent girl who was diagnostic with this disease.
Patients and Methods: • A 14 years old girl admitted with a chronic diarrhea since 4 months ,weakness ,decreased appetie and weight loss. • Physical examination showed : • A pale girl . • Fever (38.7°). • Painful abdomen. • No organomegaly or lymphomegaly . We completed with a biologic and radiologic investigation.
Results: • Laboratory investigation revealed: • elevated erythrocyte sedimentation rate(110/130) • anemia (Hb=8.7g/dl) , • high CRP (97mg/l) . • All other routine biochemical tests, celiac serology ,anti Dnatif , antinuclear anticorps were within the normal range in the serum. • The BK search was negative.
Results: • The chest X ray was normal . • Abdominal ultrasonographie showed a little ascite. • TDM showed: • ascite . • small bowel thichening. • Multiples necrotic lymphadenopathy. • liver nodule (22 mm in the segment IV)
Results: • laparotomymultiple smalls nodules and fibrotic adhesive bands covering peritoneal surfaces compatible with peritoneal tuberculosis later confirmed histologically (caseatinggranulomas) • The girl was treated with quadritherapie : Rifampicine, Izoniasid, Pyrazinamide and Ethambutol during 4 months. • There were no clinical amelioration, and a cutaneous fistulas appeared.
Results: • Myelogramme was normal. • A second abdominal TDM: showed the persistence of the same pathologie and appearing of cutaneous fistulas. • we suspected a multidrug resistant tuberculosis so we added ofloxacine , Amikacine and corticotherapie. • After 1 month the patient became more better.
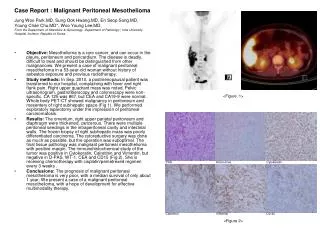
Results: Small bowelthikhening Ascite Abdominal TDM of our patient
DISCUSSION : • Peritoneal tuberculosis is predominantly a disease of young adults between 21-40 years old with an equal sex incidence. • Tuberculosisbacteriareachs the gastrointestinal tract via: • Haematogenousspread • Ingestion of infectedsputum • Direct spreadfrominfectedcontiguouslymphnodes or fallopian tubes
DISCUSSION : • Peritonealtuberculosisoccurs in threeforms : Wet type withascitis+++ Dry type withadhesions. Fibrotic type withomentalthickening and loculated ascites . • It is commonly manifested by : abdominal pain , diarrhea, fever , weight loss , and anemia. • Laboratory Findings are: Anemia , elevated sedimentation rate , high CRP. Elevated CA-125
DISCUSSION : • Chest X ray search a pulmonary tuberculosis. • Ultrasonographie ascites , lymphadenopathy, omental thickening and caking. • TDM Three main types : Wet Type Peritonitis : • Is the most common type of peritonitis (90% ). • Free or loculatedascites, • Usually slightly hyperattenuating (20–45 HU) relative to water due to its (high protein and cellular content) .
DISCUSSION : Wet type tuberculous peritonitis. Contrast-enhanced CT scan shows ascites (arrows) that is hyperattenuating relative to urine within the bladder (arrowheads)
DISCUSSION : Fibrotic Type Peritonitis: • It accounts for 60% of cases of peritonitis . • It manifests as mottled low-attenuation masses with nodular soft-tissue thickening . • Dry Type Peritonitis : • Is seen in 10% of cases. • Characterized by mesenteric thickening, fibrous adhesions, and caseous nodules. • Its imaging manifestations are highly suggestive of, but not specific for, tuberculosis.
DISCUSSION : Fibrotic type tuberculous peritonitis. CT scan obtained with oral and intravenous contrast material shows omental caking (arrowheads) with thickening of the underlying small bowel (*).
DISCUSSION : • Peritoneal Biopsy : • 85-95% Sensitive • Performed by: - laparoscopic guidance or minilaparotomy - exploratory laparotomy. • CaseatingGranulomas • Langerhans Type Giant Cells. • Microbiology Ziehl-Neelsen Stain
Treatment • Sametreatment as pulmonary TB • Four drugregimen: – Isoniazid – Rifampicin – Ethambutol – Pyrazinamide • Quadritherapieduring 2mounths thanbitheraphieduring 4moutns(Isoniazide+Rifampicin)
Conclusion : • The diagnostic of peritoneal tuberculosis is difficult. • It presents with nonspecific symptoms. laboratory investigations may not be helpful. • Radiologic investigation and laparotomy help to get the diagnostic and to treat early affected patients.