Download
1 / 6
110 likes | 421 Views
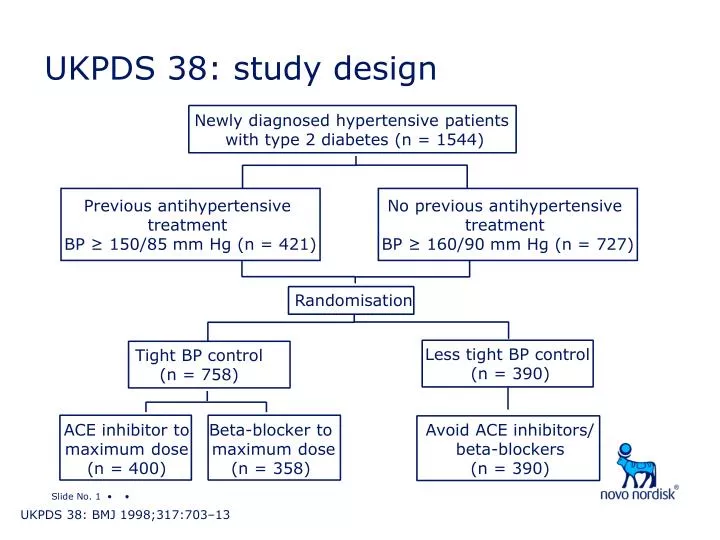
UKPDS 38: study design. Newly diagnosed hypertensive patients with type 2 diabetes (n = 1544). Previous antihypertensive treatment BP ≥ 150/85 mm Hg (n = 421). No previous antihypertensive treatment BP ≥ 160/90 mm Hg (n = 727). Randomisation. Less tight BP control (n = 390).

E N D
UKPDS 38: study design Newly diagnosed hypertensive patients with type 2 diabetes (n = 1544) Previous antihypertensive treatment BP ≥ 150/85 mm Hg (n = 421) No previous antihypertensive treatment BP ≥ 160/90 mm Hg (n = 727) Randomisation Less tight BP control (n = 390) Tight BP control (n = 758) ACE inhibitor to maximum dose (n = 400) Beta-blocker to maximum dose(n = 358) Avoid ACE inhibitors/ beta-blockers (n = 390) UKPDS 38: BMJ 1998;317:703–13
UKPDS 38: participant characteristics UKPDS 38: BMJ 1998;317:703–13
Systolic BP Diastolic BP 165 96 Tight 94 Less tight 160 92 90 155 88 86 150 84 145 82 80 140 78 0 0 Baseline 9 years Baseline 9 years UKPDS 38: tight control had a greater effect on blood pressure Blood pressure (mm Hg) UKPDS 38: BMJ 1998;317:703–13
UKPDS 38: relative risk reduction with tight blood pressure control Peripheral vascular disease Microvascular endpoint Any diabetes endpoint All-cause mortality Diabetes death MI Stroke Relative risk reduction tight vs less tight BP control(%) * p < 0.05 ** p < 0.01 ** * ** * UKPDS 38: BMJ 1998;317:703–13
160 60 Captopril Systolic Atenolol 50 140 Captopril 40 Atenolol 120 30 Absolute risk(events/1000 patients years) Blood pressure (mm Hg) 20 100 Diastolic 10 80 0 0 PVD 0 1 2 3 4 5 6 7 8 9 MI Stroke Microvascular Years from randomisation Diabetes death UKPDS 39: similar effects of beta-blocker and ACE inhibitor Any diabetes endpoint Adapted from: BMJ 1998;317:713–20
20 Captopril 18 Atenolol 16 14 12 10 8 6 4 2 0 GI Cough Headache Increasedcreatinine Impotence Depression Intermittent claudication Bronchospasm Allergic reaction Dizzy, tired, unwell UKPDS 39: reasons for non-compliance Non-compliant patients (%) UKPDS 39: BMJ 1998;317:713–20