Download

1 / 30
300 likes | 454 Views
Economics, Ethics and health Care Funding. Craig Mitton, PhD Faculty of Health and Social Development, UBC-O Centre for Healthcare Innovation & Improvement, CFRI. Outline of Session . Background to priority setting Economic framework: overview Practical steps Key concepts

E N D
Economics, Ethics and health Care Funding Craig Mitton, PhD Faculty of Health and Social Development, UBC-O Centre for Healthcare Innovation & Improvement, CFRI
Outline of Session • Background to priority setting • Economic framework: overview • Practical steps • Key concepts • Expected benefits • A bit on ethics • Activity in Canada and elsewhere
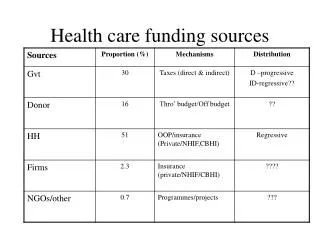
Background: scarcity • Allocation of health care funds according to defined populations is a global phenomenon • Basic notion is that of a fixed funding envelope – not enough to meet all needs $ Services = Claims on Resources Resources
Levels of Priority Setting • Provincial or state level • Health authorities • Hospitals • Program areas • Individual services • Bedside
Background: surveys • Surveys in various countries have reported feelings of inadequacy amongst decision makers for priority setting • United Kingdom (late 1990s) • Australia (2003) • Canada (late 1990s, 2004, 2005) • Unclear what tools are available assist in such activity • Consistent approaches to priority setting often not taken
Common Approaches • Historical/ political allocation: funding based on last year’s budget with some adjustments • Can become: ‘whoever yells the loudest’ • Continual growth in budgets • Other approaches: • Needs assessment, core services • Fail to consider basic economic principles
Economic principles • Opportunity cost: • By investing in program A, some benefit lost by not investing in program B… • Lost benefit of the next best alternative use of resources is the opportunity cost • Need to weigh out costs and ‘benefits’ of service options
Economic principles • The margin: • about the next unit of resources • if I had $1.00 where would I invest that dollar… • if my budget was to reduce by $1.00 where would I find that dollar… • make the most of the available resources (regardless of how much is in the total pot)
Implications of the principles • To do more of some things, we have to take resources from elsewhere, by either: • doing the same things at less cost; or • taking resources from areas of (effective) care • Measure costs and benefits of health care • Often about how much rather than whether
Economic approaches • Compare benefits from programs funded to resources required • Economic evaluation • More pragmatic but still based on the same underlying principles • Program budgeting and marginal analysis
PBMA • Framework to assist decision makers in making choices around limited resources • Used in health care since 1970s • Currently being used in health authorities in Alberta and British Columbia • Can be combined with ethical approaches in its application and is as evidence based as time and data allow for
From principles to practice 1. What resources are available in total? 2. In what ways are these resources currently spent? 3. What are the main candidates for more resources and what would be their effectiveness? 4. Are there any areas of care which could be provided to the same level of effectiveness but with less resources, so releasing resources to fund candidates in (3)? 5. Are there areas of care which, despite being effective, should have less resources because a proposal in (3) is more effective (per $ spent)?
PBMA: Practical Steps • Determine aim and scope of activity • Identify and map resource use • Form an advisory panel • Define and weight decision making criteria • Identify options for service growth and resource release • Evaluate proposed investments and disinvestment • Validate results, recommendations for (re)-allocation, communicate decisions • Evaluation, refinement and ongoing revision
Key Concepts • Shifting or re-allocating resources based on explicit comparison of options against the criteria • Single group generating expansion/ reduction options • Incentives to encourage participation • Clinicians and managers working together • Tool that supports decision making
Benefit measurement • Approach generally depends on scope of activity and resources available • Clinical outcomes • QALYs, DALYs, WTP, DCE • Multi-attribute decision analysis (MCDA) • MCDA has a long history in other sectors • Limited ‘real’ health care examples published • Fits with decision maker perspective
MCDA rating and scoring • Score service options for investment and resource release in terms of benefits for patients under pre-defined set of criteria • E.g., on a scale of 1 to 10 how geographically equitable is service Y? • To get a single measure of each service’s benefit need to combine the scores • Assuming a linear function, can add the scores taking into account criteria weights
PBMA: Outcomes Primary benefit from PBMA • Achieving real resource shifts that are consistent with strategic decision-making objectives Secondary benefit from PBMA Changes in decision making culture, evidence base Defining objectives and programs Ownership of planning process Transparent and defensible decision making Clinician engagement and partnership
Potential Challenges • Data and time requirements • Benefit measurement and relative value • Mis-alignment of incentives • Re-allocation of resources… • BUT these are always a problem in health care!! • Managers and docs alike tend to want more formal, explicit, transparent method for priority setting and resource allocation
Incorporating ethics • Ethical framework • accountability for reasonableness • Has gained momentum the last few years • hospitals, technologies, drugs • Focus is on ensuring that the chosen process of priority setting is fair and legitimate • Based on four ethical conditions
‘fair process’ • What evidence, reasons and principles are used and where did they come from? • Who is involved in the process, what communication plans were used? • What mechanisms allow for revisiting of decisions if new evidence arises? • How will decision makers ensure the process was fair? • Economics and ethics have different focuses… both can contribute to priority setting activity
Canadian PMBA examples • Chinook Health Region (AB) • Surgery, chronic disease • Headwaters Health Authority (AB) • Surgery, long term care • Calgary Health Region • Macro, children’s services • Vancouver Island Health Authority • Macro, within portfolios • Interior Health Authority • Community care services • Northern Health Authority • Home and community care
Northern Health Authority • Scope: all non-hospital H&CC services • Participants: range of clinicians, managers and finance personnel • Objective: recommendations for allocation and re-allocation to impact 2007/08 budget year • Timeline: • May 17 – decision maker training workshop • June – form advisory panel • July – formulate and validate decision criteria • Aug/ Sept – generate investment and release options • Sept. 26 – decision making retreat • Oct. – recommendations to Executive • Nov/ Dec. – evaluation and process refinement
Home & Community Care • Criteria defined and assigned weights • Health gain, access, appropriateness, strategic alignment • Scoring of proposals for investment and resource release on quantitative score sheet • Scores entered into decision analysis software • Transferred to excel to present benefit scores • Recommendations for re-allocation, endorsed by Senior Executive • Evaluation and refinements for next year
Home & Community Care • Evaluation • add in a criteria on innovation • improved vetting of original business cases • greater focus on re-allocation • BUT implemented in relatively short time, engagement perceived to be high, and process viewed as improvement over previous historical/ political allocations • additional time would allow for greater use of evidence and more in-depth analysis of proposals
International applications • Approaching close to 100 exercises in over 80 health organizations • England, Scotland, Wales, NZ, Australia, over the last 3 decades • Wide range of program areas, majority at micro/ meso levels; more recently macro level applications • Distinct shift from focus on ‘efficiency’ to more of a management process aimed at re-allocating resources to better meet wide range of organizational objectives
International applications • South West Area Health Service (WA) • Initial enthusiasm, training and survey work • Lack of leadership prevented moving forward • Waitemata District Health Board (NZ) • Internal champion, training for both macro level exercise and within Mental Health • Process carried out BUT… • Challenges in understanding business case approach • Lack of evidence due to rushed completion • Laid back CEO, lacked highest support
International lessons Clear messages Need for involving multiple stakeholders Incorporating ethical frameworks Understanding of organisational behaviour and context Leadership is everything Watch out for (major) organizational instability
Summary • Despite challenges, decisions have to be made with or without an explicit approach to priority setting • PBMA can assist decision makers in thinking about economic principles and re-allocating resources • Lots of examples of PBMA implementation and evaluation in Canada and elsewhere
Acknowledgements Michael Smith Foundation for Health Research and Canada Research Chairs program Craig.mitton@ubc.ca