Download
1 / 44
450 likes | 953 Views
USING ELECTRICAL STIMULATION TO RESTORE FUNCTION TO PARALYZED MUSCLES. William Durfee Department of Mechanical Engineering University of Minnesota Kurt Korkowski, Ben Dunn, Karl Oberjohn, Brent Harrold Department of Mechanical Engineering University of Minnesota

E N D
USING ELECTRICAL STIMULATION TO RESTORE FUNCTION TO PARALYZED MUSCLES William Durfee Department of Mechanical Engineering University of Minnesota Kurt Korkowski, Ben Dunn, Karl Oberjohn, Brent Harrold Department of Mechanical Engineering University of Minnesota Michael Goldfarb, Heather Beck Karen Palmer, Jeff Chiou Department of Mechanical Engineering Massachusetts Institute of Technology Gary Goldish, Rich Scarlotto Physical Med. & Rehab. Service VA Medical Center, Minneapolis, MN Allen Wiegner, Nancy Walsh Spinal Cord Injury Service VA Medical Center, West Roxbury, MA
u F x,v HUMAN/MACHINE DESIGN LAB Department of Mechanical Engineering University of Minnesota(www.me.umn.edu/divisions/design/hmd/) Haptic interfaces for virtual product prototyping Muscle mechanics Smart orthotics + electrical stimulation for gait restoration
OUTLINE • What is Functional Electrical Stimulation (FES)? • How FES can be used to restore motion • State-of-the-art • Why it’s hard • Commercial products • FES research at the U: • FES + "smart" orthosis • Modeling and control
FES APPLICATIONS • Bladder stimulation (incontinence) • Cerebellar stimulation (movement disorders) • Sensory substitution • Visual prostheses (blindness) • Auditory prostheses (deafness) • Pain suppression (TNS) • Pacemakers • Limb control (paralysis)
NUMBERS 150,000 in U.S. 8,000 new cases each year 1/2 quadriplegic, 1/2 paraplegic LEADING CAUSES Automobiles Guns Sports (diving) Falls SPINAL CORD INJURY AGE GROUP Range: 15-29 Mean: 23
NUMBERS 150,000 in U.S. 8,000 new cases each year 1/2 quadriplegic, 1/2 paraplegic LEADING CAUSES Automobiles Guns Sports (diving) Falls SPINAL CORD INJURY AGE GROUP Range: 15-29 Mean: 23
New Mobility, June 1997 This is the story…...of the multimillion-dollar functional electrical stimulation (FES) project that got them walking….. It's about an ambitious but flawed technology and of questionable medical ethics. And it's about a tightknit research community so convinced of its promise that it would tolerate less-than-acceptable standards of care for its human subjects. Wired For Walking: BY Sam Maddox Fifteen years ago, Bassam "Sam" Khawam, a 22-year-old Lebanese American living in the Cleveland suburbs, was paralyzed at T8-9 by a bullet. Khawam was big and physical, a black belt in karate. He was given the usual spinal cord injury prognosis: Get used to the chair, son, you're not going far without it. Khawam took the news the way many young, strong guys who join the gimp world do. He didn't buy it. "You are 22 and it happens to you," says Khawam, now a rehab engineer and father of two in Spokane, Wash. "You would want to walk again too." This is the story of Khawam and of a handful of other paralyzed research subjects, of the multimillion-dollar functional electrical stimulation (FES) project that got them walking, and of the scientist who lined up the money and ran the lab. It's a story of good intentions and good press on the side of science, and bad luck and bad faith as seen by the project's participants. It's about an ambitious but flawed technology and of questionable medical ethics. And it's about a tightknit research community so convinced of its promise that it would tolerate less-than-acceptable standards of care for its human subjects. Inside Khawam's legs is a virtual birdnest of corroding electrodes that cannot be removed without destructive surgery. He has had infections requiring antibiotics, plastic surgery and hospitalization. He and his doctors see a clear link between the infections and the electrodes, and one doctor suggested removing all of Khawam's thigh and calf muscle as the only way to get the hardware out. Another offers this bleak statement: "Mr. Khawam's prognosis is decidedly poor, as the future course of medical treatment may include either above-or below-the-knee amputation to rid him of a constant source of infection." Inside Khawam's legs is a virtual birdnest of corroding electrodes ….. He and his doctors see a clear link between the infections and the electrodes….."Mr. Khawam's prognosis is decidedly poor…..either above-or below-the-knee amputation….."
IS IT LIKE A BIPED ROBOT? (The UNH Robot Lab, www.ece.unh.edu/robots/rbt_home.htm)
CONTROLLER MOTORS SEGMENT DYNAMICS/KINEMATICS ROBOT CONTROL Commands SENSORS Disturbances Desired Task
CNS PROCESSOR BRAIN SPINAL VISUAL VESTIBULAR ? ? NATURAL SENSORS MUSCLES UPPER LIMB SEGMENT DYNAMICS/KINEMATICS CONTROLLER NATURAL SENSORS SPINAL CIRCUITS MUSCLES ARTIFICIAL SENSORS LOWER LIMB SEGMENT DYNAMICS/KINEMATICS FES CONTROL Cognitive feedback Commands Disturbances Spinal Lesion Disturbances Desired Task
SERVOMOTORS AS ACTUATORS Torque Torque Current Speed Linear, time-invariant
MUSCLES AS ACTUATORS High power/weight, but nonlinear, time-varying and uni-directional
Not enough muscles Not enough sensors Muscle force too low Muscle fatigue Spasticity Weight constraints Size constraints Cosmetic constraints Ease-of-use constraints Reliability Implanted systems No sensory feedback User control? WHAT MAKES FES DIFFERENT?
Complex system Multi-link inverted pendulum Nonlinear, time-varying actuators (muscles) Better models Better control Use model for: Designing "generic" controllers Prescribing/tuning custom systems Inputs CONTROL STIMULATOR Measurements WHY MODEL?
MODEL VERIFICATION • Direct comparison with experimental data • Predictive capability • Parameterization to the subject
MODELING FOR CONTROL OF GAIT • Rigid body links (10) • Ideal joints • Passive torques • Active torques (muscles)
u F x,v u Active (AE) K SE CE K P B P Passive (PE) MODELING MUSCLE “Muscle” = activity from single stim channel Joint-space model --> no knowledge of anatomy needed 3 inputs (u,x,v), 1 output, modified Hill-type model
ISOMETRIC MUSCLE Hammerstein model force stim Static nonlinearity Linear dynamic system Identify LDS with impluse response Identify SL by deconvolution
u Active Element F Activation Dynamics u IRC (2nd order) x,v X CE Force-Length X V CE Force-Velocity Fscale S Passive Element PE Force-Length X S PE Force-Velocity V MODELING MUSCLE Force
X MT X X SE CE CE K SE WHAT'S WRONG WITH THE MUSCLE MODEL • Invariant F-A, F-L, F-V (no change with activation) • Invariant twitch dynamics (uniform fiber types) • Time-invariant (no fatigue) • Zero neural time-delay • Rigid SEC
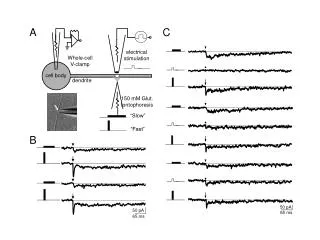
(Abushanab: Ph.D. Thesis, MIT, 1995) INTACT, HUMAN MUSCLE
40 40 Hip flexion (deg) Knee flexion (deg) 30 20 20 0 0 2 4 6 8 0 2 4 6 8 Time (sec) Time (sec) Experiment Simulation EXPT VS. MODEL
WHERE WE ARE WITH MODELING & IDENTIFICATION • Goal of modeling: simulation matches experiment • Subject-to-subject variation is large ==> calibration is required • How good is "good enough" will be determined by control strategy • Must extend to subjects with SCI • Better experimental ID methods evolving • More diverse verification tests evolving
PROBLEMS WITH FES-AIDED GAIT Requires precise, stable control for repeatable steps Muscles are nonlinear, time-varying (1) Need to walk for reasonable distances Muscles fatigue rapidly (2) PROPOSED SOLUTION: Stimulation plus "smart" orthotics
Designed for RESEARCH use CBO OVERVIEW, SPECIFICATIONS • JOINTS • 2-dof hip, 1-dof knee, fixed ankle • hip adduction stop • magnetic particle brakes • Evoloid gear, 16:1 transmission • STRUCTURE • aluminum, chromoly • WEIGHT, INERTIA • 12.5 lbs, 10% of limb inertia • STIMULATION AND CONTROL • 4-channel stimulation • on/off stimulation control • closed-loop brake control (Goldfarb and Durfee, IEEE Tran Rehab Eng, 4(1):13-24, 1996)
CBO EVALUATION PROTOCOL • 4-channel stimulation (quad + peroneal) • Parallel bars, walker 5 - 10 m lengths • Compare gait with and without CBO • Speed/distance, quadriceps use, repeatability • Four subjects with paraplegia
FES FES + CBO
0.14 60 0.12 50 0.1 40 0.08 30 0.06 20 0.04 10 0.02 0 0 Without CBO With CBO Without CBO With CBO INCREASED SPEED, DISTANCE Gait Speed Gait Distance 50 0.12 0.09 25 Distance (m) Speed (m/s)
OPEN ISSUES • Substantial improvement in FES-aided gait.....but preliminary, laboratory results only • Consumer-driven design (size, weight, ease of use) Technical issues Commercialization issues Handling upper-limb inputs ??? Market size ??? Startle, stumble response ??? User acceptance ??? Fault tolerant equipment ??? Who pays !!??