Download
1 / 43
430 likes | 656 Views
Coagulopathies in the Critical Care Setting . Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CNRN, CEN, NP Education Specialist LRM Consulting Nashville, TN. Coagulopathies in the Critical Care Setting . Objectives

E N D
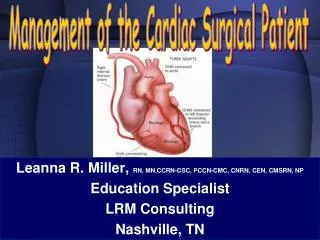
Coagulopathies in the Critical Care Setting Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CNRN, CEN, NP Education Specialist LRM Consulting Nashville, TN
Coagulopathies in the Critical Care Setting • Objectives • Identify the most likely type of coagulopathy with regards to INR, aPTT, platelet numbers and function. • Discuss the four causes of thrombocytopenia. • Describe the priorities in the management of patients with life – threatening coagulopathies.
Coagulopathies in the Critical Care Setting Admission Screening • identify defects in hemostasis that can be corrected • guide the management of hemostatic defects that cannot be corrected • help manage the bleeding that cannot be prevented
Coagulopathies in the Critical Care Setting Preoperative Screening • History & Physical unlikely congenital or familial coagulopathy • no personal or family history of bleeding • no abnormal bleeding associated with: • dental extractions • previous surgery • routine childhood trauma
Coagulopathies in the Critical Care Setting Preoperative Screening • CBC • Hgb/Hct • platelets • PT/PTT • Bleeding Time
Coagulopathies in the Critical Care Setting Admission Screening • Assessment of Coagulopathy • CBC with coagulation studies • check for and correct hypothermia • review the history • review medications
Coagulopathies in the Critical Care Setting Postoperative Bleeding • Vascular integrity disruption • reoperation
Coagulopathies in the Critical Care Setting Medical Causes of Bleeding • residual heparin effect • platelet consumption (CPB) • preoperative platelet inactivation
Coagulopathies in the Critical Care Setting Protamine Reactions • Type I • benign reaction • Histamine release systemic hypotension • administer protamine slowly
Coagulopathies in the Critical Care Setting Protamine Reactions • Type II • anaphylactoid reaction • occurs within 10 to 20 minutes of administration • symptoms • hypotension • flushing • edema • bronchospasm
Coagulopathies in the Critical Care Setting Protamine Reactions • Type III • catastrophic pulmonary vasoconstriction • elevated pulmonary pressures • cardiopulmonary collapse • noncardiogenic pulmonary edema • reaction occurs between 10 to 20 minutes after start of administration
Coagulopathies in the Critical Care Setting Medical Causes of Bleeding • depletion of clotting factors • pre-existing coagulopathy • fibrinolysis
Coagulopathies in the Critical Care Setting • Thrombocytopenia • platelet destruction • drug – induced • DIC
Coagulopathies in the Critical Care Setting Differential diagnosis • A platelet count fall that begins 5 to 10 days after cardiac surgery or that occurs abruptly after starting heparin in a patient previously exposed to heparin within the past 5 to 100 days, is very suggestive of HIT.
Coagulopathies in the Critical Care Setting • Thrombocytopenia • Etiology • abnormal distribution or sequestration in spleen • portal hypertension
Coagulopathies in the Critical Care Setting • Thrombocytopenia • Etiology • dilutional after hemorrhage, RBC transfusions
Coagulopathies in the Critical Care Setting • Thrombocytopenia • Diagnosis • hemoglobin,hematocrit, platelets • prolonged bleeding time, PT, PTT
Coagulopathies in the Critical Care Setting Disseminated Intravascular Coagulation Definition • serious bleeding disorder • thrombosis; then hemorrhage
Coagulopathies in the Critical Care Setting Pathophysiology • Intrinsic Clotting Cascade • endothelial injury • assessed by PTT
Coagulopathies in the Critical Care Setting Pathophysiology • Extrinsic Clotting Cascade • tissue thromboplastin • assessed by PT
Coagulopathies in the Critical Care Setting Etiology of DIC • Obstetric • abruptio placentae • amniotic fluid embolus • eclampsia
Coagulopathies in the Critical Care Setting Etiology of DIC • Hemolytic/Immunologic • anaphylaxis • hemolytic blood reaction • massive blood transfusion
Coagulopathies in the Critical Care Setting Etiology of DIC • Infectious • bacterial • fungal • viral • rickettsial
Coagulopathies in the Critical Care Setting Etiology of DIC • Vascular • shock • dissecting aneurysm
Coagulopathies in the Critical Care Setting Etiology of DIC • Miscellaneous • Emboli (fat) • ASA poisoning • GI disturbances - pancreatitis
Coagulopathies in the Critical Care Setting Laboratory Findings • platelets • fibrinogen • PT &/or PTT • d - dimer or FSP • ATIII
Coagulopathies in the Critical Care Setting Management • Treat underlying cause • surgery • antimicrobials • antineoplastics
Coagulopathies in the Critical Care Setting Management • Stop Thrombosis • IV heparin • AT III • plasmapheresis
Coagulopathies in the Critical Care Setting Management • Administer blood products • pRBCs • platelets • FFP • cryoprecipitate
Coagulopathies in the Critical Care Setting Complications • hypovolemic shock • acute renal failure • infection • ARDS
Coagulopathies in the Critical Care Setting Postoperative Bleeding • Platelet Dysfunction • Platelets • FFP/cryoprecipitate • DDAVP
Coagulopathies in the Critical Care Setting Postoperative Bleeding • Coagulation Factor Deficiency • FFP/cryoprecipitate • protamine
Coagulopathies in the Critical Care Setting Postoperative Bleeding • Hyperfibrinolysis • DDAVP • Antifibrinolytics • Amicar
Coagulopathies in the Critical Care Setting Case Study • 62 – year old male • admitted to CVICU post bypass • complications postop (tamponade) – stabilized & on IABP • required CPR several times
Coagulopathies in the Critical Care Setting Case Study • 3 days later diminished leg circulation – IABP removed • pneumonia, groin infection, renal failure • step – down develops sternal wound infection
Coagulopathies in the Critical Care Setting Lab Values • ABGs pH 7.26 pO2 55 pCO2 52 HCO3 18 SaO2 84%
Coagulopathies in the Critical Care Setting CV Status BP 88/56 MAP 67 CVP 4 ECG ST T 39.2°C
Coagulopathies in the Critical Care Setting Case Study Hgb/Hct 8.8 / 30% PT 38 seconds Fibrinogen 102 mg/dL Platelets 50,000/mm3 D – dimer > 2500 ng/dL FSP 80 mcg/dL
Coagulopathies in the Critical Care Setting IN CONCLUSION