Download
1 / 14
320 likes | 1.28k Views
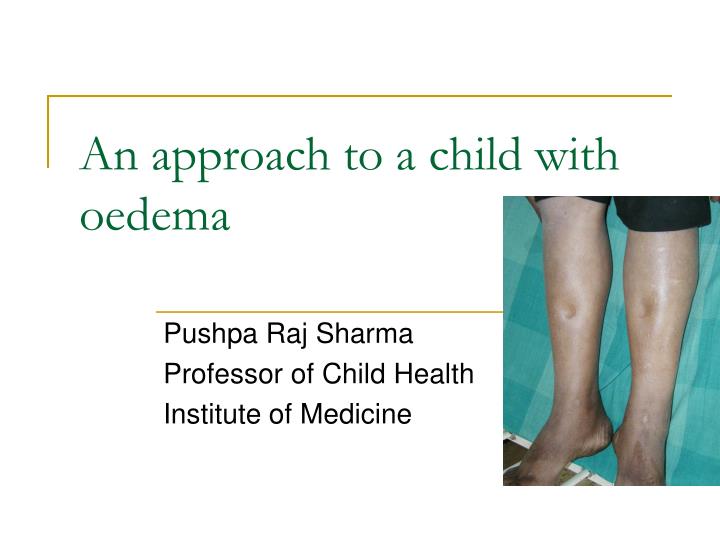
An approach to a child with oedema. Pushpa Raj Sharma Professor of Child Health Institute of Medicine. Oedema: accumulation excess interstitial fluid. Increased hydrostatic pressure Acute nephritic syndrome Congestive cardiac failure Decreased plasma oncotic pressure

E N D
An approach to a child with oedema Pushpa Raj Sharma Professor of Child Health Institute of Medicine
Oedema: accumulation excess interstitial fluid • Increased hydrostatic pressure • Acute nephritic syndrome • Congestive cardiac failure • Decreased plasma oncotic pressure • Protein calorie malnutrition, Nephrotic syndrome; protein loosing enteropathy • Increased capillary leakage • Allergy, sepsis, angiooedema. • Impaired venous flow • Vanacaval obstruction, hepatic vein obstruction • Impaired lymphatic flow • Congenital lymphedema, Wuchereria bancrofti infection
Sensitivity Specificity Understandable Open ended Leading Short Acceptable Entry questions: Enters into the organ/ system Threading question Enters into the specific aetiology. Entry questions and threading questions
Examples for formulation of questions • Localized oedema • Insect bite; trauma; skin infections • Kwashiorkar (bilateral pedal) • Superior vanacaval obstruction • Lymphatic obstruction • Orthostatic • Generalized oedema • Renal: periorbital; hematuria; hypertension; symptoms of collagen disease (rash, joint pain); frothy urine; symptoms of uraemia (vomiting, nausea, pallor), convulsion, low urine output.
Examples for formulation of questions • Cardiac: orthopnoea, joint pain; palpitation; giddiness; fainting episodes; bluish episodes; • Protein energy malnutrition: low calorie and protein in the diet for long; precipitating factors (persistent diarrhea, chronic illnesses) • Hepatic: Jaundice; ascites; prominent abdominal veins; neonatal umbilical sepsis; spleenomegaly; purpura • Collagen diseases: fever, rash, joint pain, pallor
4 year old girl, who recently recovered from a sore throat, was brought to the OPD with symptoms of swelling of both feet. Physical examination reveals edema around the eyes and the ankle. A routine urinalysis reveals the following results. First case The most likely diagnosis is
Urine examination • Chemical/Physical AnalysisColor:Yellow’ Blood:Moderate;Clarity:Hazy;pH:6.5 • Glucose:Negative;Protein:300mg/dL;Ketones:Negative • Specific Gravity:1.015 ;Nitrite:Negative • Microscopic Analysis20-50 RBC/hpf 10-20 WBC/hpf 2-5 RBC casts/hpf 2-5 Granular casts/hpf What is the most likely diagnosis?
5 year male child Swelling first noticed around eyes. No history of shortness of breath; fever; cough; jaundice; umbilical infection; no dark colored urine. Height: 110cms; Wt: 18kg; liver not enlarged; Ascites present Second case The most likely diagnosis is
!2 year male from Pokhara; arrived after traveling by bus for 12 hours. History of fever Upper abdominal pain Dark colored urine No past history of sore throat, rash, joint pain diarrhea, trauma. Comfortably lying flat in bed Oral temp: 102.0 Respiratory rate: 28.min Bilateral pedal edema, non tender Absence of Jaundice Weight: 38 Kg. Chest: normal Abdomen: Tender R hypo. No free fluid Third case
Third case: • Normal blood count • Urine: routine normal • Liver function: normal • X-ray chest: normal What causes we have excluded? Increased hydrostatic pressure? Decreased plasma oncotic pressure? Increased capillary leakage? Impaired venous flow? Impaired lymphatic flow?
Third case: further investigation • Bilateral edema and tender R hypochondrium. • Ultrasound of the abdomen: • Thickened Gall Bladder wall • Mucocoele
Third case :Final diagnosis and pathophysiology • Edema: increased hydrostatic pressure due to gravitational effect from prolonged leg hanging. • R. Hypochondrium pain and fever: cholecystitis and mucocele of gall bladder (ultrasound supported) Edema subsided on the next day after admission.
Fourth case • 5 year male child • Swelling started from limb : one month • No history of cough, shortness of breath, cyanosis, jaundice, dark colored urine, umbilical infection. • Persistent diarrhea +. • Irritable; wt: 6 kg; Ht: 100cms. Serum protein: 1.5G/dL; Urine normal What is the diagnosis?
Fourth case • 6 year female child • Swelling both feet for 10 days. • History: shortness of breath off and on for1 year, joint pain; palpitation; low urine output; fever with rigor • Tachypnoea; pyrexial, propped-up; raised JVP, enlarged liver and spleen; urine shows RBC. The most likely diagnosis is