Download
1 / 24
250 likes | 440 Views
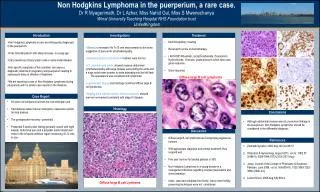
A Case of Lymphoma in IBD. David T. Rubin MD Meenakshi Bewtra , MD MPH. Case:. 28 year old white male h/o pancolitis UC diagnosed 2006, treated with: 2006: Corticosteroids , Asacol , 6MP--continued active disease 2006-2007: Infliximab—continued steroid-requirement

E N D
A Case of Lymphoma in IBD David T. Rubin MD MeenakshiBewtra, MD MPH
Case: • 28 year old white male h/o pancolitis UC diagnosed 2006, treated with: • 2006: Corticosteroids , Asacol, 6MP--continued active disease • 2006-2007: Infliximab—continued steroid-requirement • 2007-2009: 6MP—incomplete response; continued steroid-requirement • 2009: C.difficle infection • 2011: adalimumb—incomplete response; continued steroid-requirement • 2012: carbohydrate diet; Salmonella infection • In 2012, diagnosed with HL • Currently treated with ABVD; continues on prednisone • Flex sig and colonoscopy: inflammation in rectosigmoid
Case (con’t): • PMHx/PSHx: otherwise unremarkable • FamHx: colorectal cancer (maternal grandfather); non-melanoma skin cancer (maternal grandfather, mother) • SocHx: non-smoker • ROS: otherwise non-contributory • PE: unremarkable • Pathology: • WBC 18; Hgb 9.2; Hct 30.7; Plt 648; Alb 3.3; AlkPhos 152; ALT 97; AST 44 • Most recent flexible sigmoidoscopy: rectosigmoid biopsies—severely active UC with necrotic exudate.
Outline: • Baseline risk for lymphoma in IBD • Mechanism for lymphoma development in immunosuppression • Published risks of lymphoma for IBD immunosuppressant medications • What to do next?
IBD and lymphoma: baseline risk? • Population-based cohorts or • Tertiary centers: • Closer surveillance • Over-reporting • Earlier diagnosis • Longer duration of disease • Increased use of immunosuppression • Confounding due to co-existing diseases
IBD and lymphoma: baseline risk? • Loftus et al Am J Gastroenterol 2000;95:2308–12 • Olmstead County 1940-1993: 1 NHL in 6662 IBD patient-years (crude risk 0.002) • Mayo Clinic 1976-1997: 61 NHL in 15,000 patients seen (crude risk 0.004) Bewtra M, and Lewis JD Gastroenterol Clin N Am 38 (2009) 669–689
IBD and lymphoma: baseline risk? • Potentially a higher risk of lymphoma in IBD • Tertiary care centers • Numerous limitations/confounders • Despite this, the absolute risk remains LOW • General population age-adjusted annual incidence of lymphoma (SEER): 20 per 100,000
Outline: • Baseline risk for lymphoma in IBD • Mechanism for lymphoma development in immunosuppression • Published risks of lymphoma for IBD immunosuppressant medications • What to do next?
Mechanism for lymphoma development • Defective immune system = increased risk of lymphoma • Defective immunologic tumor cell surveillance • Specifically implicated in Epstein-Barr (EBV) virus-positive lymphoma • Human herpes virus infection in >90% of population • Immunosuppression allows emergence of lymphoproliferative disorders associated with EBV
Outline: • Baseline risk for lymphoma in IBD • Mechanism for lymphoma development in immunosuppression • Published risks of lymphoma for IBD immunosuppressant medications • What to do next?
Cyclosporine: • Most experience/evidence from transplant and dermatology literature • Case reports only in IBD literature • Confounded by multiple medications Cockburn et al. J Autoimmun1989;2:723–31 Paul et al. J Invest Dermatol2003;120: 211–6
Methotrexate: • Limited data in IBD • Lack of sample size and follow-up time • Confounding by other medications • Psoriasis and RA: more experience abased on patients with >36 months exposure to MTX Bewtra M, Lewis JD, Expert Rev ClinImmunol. 2010 bbased on patients with <36 months exposure to MTX Jul;6(4):621-31
Azathioprine/6-MP: 1:4,357 (age 20-29) 1:355 (age > 65) Bewtra M, Lewis JD, Expert Rev ClinImmunol. 2010 Jul;6(4):621-31
Azathioprine/6-MP: • CESAME study Beaugerie L et al. Lancet 2009
Riskof LymphomaReturns to Normal afterStoppingThiopurines • 36,891 VA patients with UC with a median follow up of 6.7 years and a median age of 60 years at inclusion • 4,734 patients using thiopurines; median duration of exposure : 0.97 years • 142 confirmed lymphoma cases Khan, N. et al. Presented at DDW May 2013. Abstract Mo641.
Anti-TNFs: • Meta-analysis (infliximab, adalimumab, certolizumab): • Combination immunosuppression: • SIR 6.6 (4.4-8.8) to SIR 10.2 (1.2-36.9) Siegel C. et al. Clin Gastro Hep 2009 Herrinton Am J Gastro 2011 Beaugerie, Lancet 2009
Combination Therapy: (1) Beaugerie et al, Lancet 2009 (2) HerrintonAm J Gastro 2011
Hepatosplenic T-Cell Lymphoma • Extranodal T-cell lymphoma • Not EBV-related • Ochenrider et al. Clin Lymphoma Myeloma Leuk. 2010;10(2):144-148 • 28 cases reported, all in CD • All exposed to thiopurine • 22 exposed to anti-TNF therapy • 3 in patients treated with adalimumab • Majority (93%) male • Median age: 22 years old • Herrinton L et al, Pharmacoepi Drug Safety 2012: • 0.3 (95%CI, 0.11–0.65) per million person- years (baseline population) • 48 per million-person years (1 case reported) • 1: 20,964
Hepatosplenic T-Cell Lymphoma • In patients < 35 years of age: • Risk of thiopurinemonotherapy: 1:7,404 • Risk of combination therapy: 1:3,534 Parakkal D et al, Eur J Gastro and Hep 2011
Outline: • Baseline risk for lymphoma in IBD • Mechanism for lymphoma development in immunosuppression • Published risks of lymphoma for IBD immunosuppressant medications • What to do next?
After diagnosis of lymphoma:Consult Oncology. • Continue therapy: • Previously treated lymphoma and inactive > 1 year • Stop therapy: • New lymphoma • EBV+ on 6-MP • If HSTCL, avoid future 6MP (? anti-TNF)