Download
1 / 49
560 likes | 882 Views
Nephroprotection: Actual perspective of ACE inhibitor therapy Piero Ruggenenti Mario Negri Institute for Pharmacological Research Bergamo, Italy Malaga, October 10, 2005. 1,800,000 patients with ESRD. J. Weening, G. Remuzzi, Lancet, 2005. 90 %. DIALYSIS POPULATION. GLOBAL MAINTENANCE.

E N D
Nephroprotection: Actual perspective of ACE inhibitor therapy Piero Ruggenenti Mario Negri Institute for Pharmacological Research Bergamo, Italy Malaga, October 10, 2005
1,800,000 patients with ESRD J. Weening, G. Remuzzi, Lancet, 2005
DIALYSIS POPULATION GLOBAL MAINTENANCE TEN YEAR MEDICAL COSTS 2,500,000 1,200 $ 1,000 2,000,000 800 $ ( billions) 1,500,000 600 $ 1,000,000 400 500,000 200 $ 0 0 1990 2000 2010 1981-1990 1991-2000 2001-2010 Lysaght, J Am Soc Nephrol, 2002
80 60 1/Cr x 10 3(µmol/l) 40 20 0 0 10 20 30 40 50 Time(months) PROGRESSION OF RENAL FAILURE IN 9 DIABETICS Modified from Jones et al., Lancet, 1979
April 3, 1952 THE BRITISH MEDICAL JOURNAL STRUCTURAL AND FUNCTIONAL ADAPTATION IN RENAL FAILURE The seconf of two Lumleian Lectures delivered to the Royal College of Physicians of London By Robert Platt, M.D., M.Sc.,F.R.C.P., “…the functional disturbances known to occur in human renal disease are precisely those which occur in animal experiment as a result of reduction in the amount of functioning renal substance - that is, loss of nephron”
GLOMERULAR HYPERTENSION AND THE EFECT OF ACE-INHIBITORS IN EXPERIMENTAL DIABETES Control Diabetes 0 10 20 30 40 50 60 70 DP (mmHg) DP = transmembrane pressure difference Zatz et al., J Clin Invest, 1986
GLOMERULAR HYPERTENSION Mechanical strain * 1.2 2.5 1.0 2.0 Ang II (pg per µg of cell lysate) 0.8 AT1R level (adjusted for tubulin) 1.5 Podocyte number 0.6 1.0 0.4 0.5 0.2 0 0 Ctr MS Ctr MS Durvasula et al, Kidney Int, 2004 Pore dimension Proteinuria SCARRING Riser et al., Am J Pathol, 1996
PODOCYTE DYSFUNCTION IN RESPONSE TO PROTEIN LOAD Ang II ACEi / AIIRA Increased glomerular permeability to proteins Proteinuria Podocyte protein accumulation Loss of differentiated phenotype Cytoskeleton rearrangement Gene activation TGF-b Slit diaphragm dysfunction Prosclerosing activation of mesangial cells Podocyte detachment Foot process effacement Permselective dysfunction Permselective dysfunction GLOMERULOSCLEROSIS Abbate et al., Am J Pathol, 2002
PATHOPHYSIOLOGY OF PROGRESSIVE NEPHROPATHIES Renal injury Increased glomerular permeability to macromolecules Glomerular-capillary hypertension Reduction of nephron numbers Proteinuria Increased filtration of plasma proteins Excessive tubular reabsorption Nuclear signals for NF-kB-dependent and independent vasoactive and inflammatory genes. Corresponding protein products then released into interstitium Tubular cell transdifferentiation Fibroblast proliferation Fibrogenesis Renal scarring Remuzzi and Bertani, N Engl J Med,1998
ACE INHIBITION PREVENTS RENAL FAILURE AND DEATH IN UNINEPHRECTOMIZED MWF/ZTM RATS * 700 600 500 Urinary Protein Excretion (mg/24 hrs) 400 300 200 100 ** 0 Control UNx UNx + Lis * 100 Control Percentage of glomeruli affected by sclerosis 100 80 UNx + Lis 80 (%) 60 60 40 Survival 40 20 20 ** UNx 0 0 0 3 6 9 1 2 1 5 Control UNx UNx + Time (months after UNx) Lis * p < 0.05, **p < 0.01 vs control Remuzzi A. et al., Kidney Int, 1995
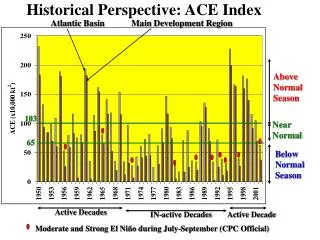
REIN CORE Rate of GFR decline according to base-line proteinuria - Interim analysis on 177 patients p=0.001 0.89±0.11 1.0 Rate of GFR decline (ml/min/month) p=0.001 1.0 0.39±0.10 Rate of GFR decline (ml/min/month) 0.5 0.67±0.08 0.5 0.25±0.08 0 Conventional Ramipril 0 STRATUM - 1 U. Prot. 1-3 g/24 h STRATUM - 2 U. Prot. ≥ 3 g/24 h Ramipril 77 % Kidney survival: Conventional 54 % GISEN Group, Lancet, 1997
REIN CORE Conventional Ramipril 1.6 70 1.4 60 Mean rate of GFR decline (ml/min/month) % patients with doubling of base-line creatinine or ESRF 1.2 50 1.0 40 0.8 30 0.6 20 0.4 10 0.2 0 0 3 - 4.5 4.5 - 7 ≥ 7 3 - 4.5 4.5 - 7 ≥ 7 Baseline proteinuria (g/24 h) Baseline proteinuria (g/24 h) GISEN Group, Lancet, 1997
INCIDENCE OF ESRD IN 352 PATIENTS WITH PROTEINURIC, CHRONIC NEPHROPATHIES ACCORDING TO TREATMENT AND TERTILES OF BASAL GFR Post-hoc analyses of the REIN study p < 0.05 70 60.0 60 50 40.4 Incidence of ESRD (%) 40 30 21.4 p < 0.01 20 Conventional 13.4 10.9 Ramipril 10 0.0 0 Middle (32.6 - 50.8) Lowest (10.5 - 32.6) Highest (50.8 - 101.0) GFR (ml/min) TERTILES Ruggenenti et al., J Am Soc Nephrol, 2002
EFFICACYAND SAFETYOF BENAZEPRILIN PATIENTS WITH ADVANCEDCHRONIC RENAL INSUFFICIENCY (ESBARI) A randomized controlled trial Patients: Inclusion criteria: Treatment: Follow-up: Outcomes Primary: Secondary: 224 subjects with non-diabetic chronic nephropathies S. creatinine: 3.1- 5.0 mg/dl Benazepril(20 mg/day) Placebo 3.4 years (mean) Doubling of s. cretinine, ESRD or death Proteinuria Hou et al., 2005
EFFICACYAND SAFETYOF BENAZEPRILIN PATIENTS WITH ADVANCEDCHRONIC RENAL INSUFFICIENCY (ESBARI) A randomized controlled trial 100 80 Benazepril 60 Patients without doubling serum creatinine,ESRD, or death (%) Placebo 40 20 0 0 12 24 36 Months of follow-up Hou et al., 2005
LESS PROGRESSION TO ANURIA IN 60 PERITONEAL DIALYSIS PATIENTS DURING 1-YEAR ACE INHIBITOR THERAPY Aprospective randomized study 100 80 60 40 20 0 Placebo Ramipril (5 mg/day) Target blood pressure: <135/85 mmHg Philips et al., J Am Soc Nephrol, 2002
ACE INHIBITORS AND SURVIVAL OF HEMODIALYSIS PATIENTS A retrospective analysis (1994-2000) at a single Institution 100 80 ACEi YES n = 60 60 p < 0.0006 Cumulative survival (%) 40 20 ACEi NO n = 68 0 0 20 40 60 80 100 months All the benefit driven by a reduced incidence of CV deaths (8 % vs 29 %, p = 0.003) in patients < 65 years-old Cardioprotection achieved despite less effective BP control Efrati et al., Am J Kidney Dis, 2002
Ramipril Ramipril 4 5 D GFR = -0.44 ± 0.54 4 0 D GFR = -0.10 ± 0.50 GFR (ml/min/month) 3 5 3 0 D GFR = -0.81 ± 1.12 D GFR = -0.14 ± 0.87 2 5 Conventional Ramipril FOLLOW-UP CORE Ruggenenti et al., Lancet, 1998
Cohorts ≥ 36 months ≥ 42 months ≥ 48 months ≥ 54 months CONTINUED RAMIPRIL 45 40 35 DGFR (ml/min/month) 30 25 -.33 -.30 -.24 -.23 -.20 -.21 -.18 -.16 -.24 -.19 -.17 20 months 0 18 30 0 18 30 42 0 18 30 42 0 18 30 42 SWITCHED RAMIPRIL 45 40 35 DGFR (ml/min/month)) 30 25 -.46 -.52 -.46 -.52 -.49 -.28 -.46 -.45 -.45 -.51 -.53 20 0 18 30 0 18 30 42 0 18 30 42 0 18 30 42 months Ruggenenti et al., J Am Soc Nephrol, 1999
-.10 CONTINUED RAMIPRIL SWITCHED RAMIPRIL Cohorts ≥ 60 months ≥ 60 months 45 40 35 DGFR (ml/min/month) 30 25 -.16 -.13 -.11 -.25 -.35 -.44 -.30 20 0 18 30 42 60 0 18 30 42 60 months months Ruggenenti et al., J Am Soc Nephrol, 1999
REGRESSION REMISSION 10 patients with increasing D GFR 16 patients with stableD GFR Change in proteinuria (post- vs pre- breakpoint) - 31 % - 52 % 90 90 80 80 70 70 60 60 GFR (ml/min/month) 50 50 40 40 30 30 20 20 10 10 0 0 0 10 20 30 40 50 60 0 10 20 30 40 50 60 months months Slopes refer to 26 patients on continuated Ramipril treatment since randomization who had at least 6 GFR measurements (≥ 3 on Core and ≤ 3 on Follow-up study) Ruggenenti et al., J Am Soc Nephrol, 1999
EVIDENCE FOR GLOMERULAR CAPILLARY REGENERATION AND REABSORPTION OF SCLEROSIS AREAS 100 MWF 60 w 80 60 100 40 MWF 50 w 80 20 60 Number of glomeruli (%) 0 0 <25 25-50 50-75 >75 % 40 100 MWF 60 w + LIS 20 80 0 60 >75 % 0 <25 25-50 50-75 % sclerotic changes 40 20 0 0 <25 25-50 50-75 >75 % Remuzzi et al., J Am Soc Nephrol, 2003
#1 #60 #80 #20 #1 #60 #100 #40 #80 #20 #100 #40 MWF 60 W MWF 50 W MWF 60 W + LISINOPRIL #1 #60 #20 #80 #100 #40
Definitions of progression, remission, and regression of proteinuric chronic nephropathies Variable Progression Remission Regression Proteinuria Glomerular filtration rate Renal structural changes ≥ 1 g/24 h Declining* Worsening < 1 g/24 h Stable Stable < 0.3 g/24 h Increasing Improving *Faster than physiological decline associated with aging (1 ml/min/1.73 sqm per year) Ruggenenti et al., THE LANCET • Vol 357 • May 19, 2001
NON-DIABETIC CHRONIC NEPHROPATHIES Ramipril (n = 20) Proteinuria GFR 3 70 2 60 g/24 hours ml/min 1 50 40 0 0 6 12 18 24 0 6 12 18 24 months months
CAN WE DO BETTER? protein traffic Up-titrate ACE inhibitor dose Intensify blood pressure control Combine with other antiproteinuric agents Vasopeptidase inhibitors Low-protein diet • - Non-dihydropyridinic Ca-channel blockers • Ang II receptor blockers • Aldosterone antagonists consequences of protein traffic Drugs targeted to inflammatory or vasoactive genes which are up-regulated by protein reabsorption • - ET-1 receptor antagonists • TGFb inhibitors • Lipid lowering agents • C3 inhibitory agents
24 h Proteinuria* M.A.P.* y=-1.23x - 12.07 0 +20 r =-1.23; p<0.02 -10 +10 0 -20 D vs. no treatment (%) -30 -10 -40 -20 -50 -30 -60 -30 0 5 10 15 20 0 5 10 15 20 Ramipril dose (mg/day) Ramipril dose (mg/day) * No correlation between proteinuria and BP changes
Blood-pressure control for renoprotection in patients with non-diabetic chronic renal disease (REIN-2): multicentre, randomised controlled trial Piero Ruggenenti, Annalisa Perna, Giacomina Loriga, Maria Ganeva, Bogdan Ene-Iordache, Marta Turturro, Maria Lesti, Elena Perticucci, Ivan Nediyalkov Chakarski, Daniela Leonardis, Giovanni Garini, Adalberto Sessa, Carlo Basile, Mirella Alpa, Renzo Scanziani, Gianbattista Sorba, Carmine Zoccali, Giuseppe Remuzzi, for the REIN-2 Study Group* Lancet 2005; 365: 939-46
REIN-2 Patients: Inclusion criteria: Treatment: Follow-up: Outcomes: 335 subjects with non-diabetic chronic nephropathies Proteinuria > 1 g/24 hours Cr. Cl. < 70 ml/min/1.73 sqm Ramipril(2.5-5 mg/day) Target DBP: < 90 mmHg Ramipril (2.5-5 mg/day) + Felodipine(5 -10 mg/day) Target S/DBP: < 130/80 mmHg 19 (I.Q.R.: 12-35) months ESRD DGFR (in a sub-group)
MEAN ARTERIAL PRESSURE IN EACH STUDY ARM 104 102 100 Ramipril Mean arterial pressure (mmHg) 98 Ramipril + Felodipine 96 94 92 90 0 3 6 9 12 15 18 21 24 Months Ruggenenti et al., Lancet, 2005
REIN-2 Ramipril + Felodipine 45 40 Ramipril 35 30 25 Subjects with ESRD (%) 20 15 10 5 0 0 6 12 18 24 30 36 42 48 54 Follow-up (months) No. at risk Usual BP Lower BP 168 167 158 155 121 126 84 88 64 59 50 51 34 43 24 31 13 17 2 0 Ruggenenti et al., Lancet, 2005
Lancet, 2005 Renoprotective therapy: is it blood pressure or albuminuria that matters? Paul E. De Jong, Dick de Zeeuw
A CASE-CONTROL STUDY OF SINGLE OR DUAL RAS INHIBITION IN PATIENTS WITH NON-DIABETIC CHRONIC NEPHROPATHIES Ramipril (n = 20) Benazepril + Valsartan (n = 20) Proteinuria GFR 3 70 2 60 * p < 0.01 g/24 hours ml/min 1 50 * * * * 40 0 0 6 12 18 24 0 6 12 18 24 months months
COOPERATE study: results 100 Combination Losartan 80 Trandolapril Patients without events * (%) 60 40 20 0 0 6 12 18 24 30 36 Months after randomisation * ESRD and doubling of serum creatinine Nakao et al., Lancet, 2003
SEVERE PASSIVE HEYMANN NEPHRITIS (UNINEPHRECTOMY) 800 Treatment for 10 months (start treatment at 2 months) 600 Urinary protein excretion (mg/day) * 400 200 * 0 80 60 Glomerulosclerosis (%) 40 * * 20 * Lisinopril Lis + AII-RA Lis + AII-RA +Cerivastatin Control Vehicle Zoja et al., J Am Soc Nephrol, 2002
REMISSION CLINIC Start low-dose sodium diet Add low-dose ACE i or AII RA Up-titrate ACE i or AII RA to max tolerated dose Add a diuretic Add a low dose of another antiproteinuric agent Add AII RA or ACE i Up-titrate AII RA or ACE i to maximum dose K > 5.5 mEq/l K < 5.5 mEq/l Add non-dihydropyridine CCBs (Verapamil/Diltiazem) Up-titrate non-dihydropiridine CCBs to max tolerated dose Up titrate concomitant antihypertensive agents to achieve the maximum tolerated blood pressure reduction Add a lipid lowering agent Ruggenenti et al., Lancet, 2001
REMISSION CLINIC Targets of the multidrug approach: Blood pressure < 120/80 mmHg Proteinuria < 0.3 g/24 h LDL < 100 mg/dl LDL + VLDL < 130 mg/dl HbA1c < 7.5 % (diabetics) Ruggenenti et al., Lancet, 2001
- Full remission of nephrotic syndrome (U.prot. <1g/24 h) in 25 patients - Stable s. creatinine 5 8 Remission clinic 4 6 Urinary protein excretion (g/24 hours) 3 Serum creatinine (mg/dl) 4 2 2 1 0 0 24 - 50 0 6 12 18 24 - 12 - 6 months
- Residual proteinuria > 1g/24 h in 11 patients Remission clinic 5 8 * 4 6 Urinary protein excretion (g/24 hours) 3 Serum creatinine (mg/dl) 4 2 2 1 0 0 > 24 0 6 12 18 24 - 12 - 6 months * 2 patients progressed to ESRD
TYPE 2 DIABETES FULL-RESPONDERS (n=5) - Full remission of nephrotic syndrome (U.prot. <1g/24 h) - Stable s. creatinine 3 8 Remission clinic 6 2 Serum creatinine (mg/dl) Urinary protein excretion (g/24 hours) 4 1 2 0 0 > 24 0 6 12 18 24 - 6 months
TYPE 2 DIABETES PARTIAL-RESPONDERS (n=13) - Residual proteinuria > 1g/24 h Remission clinic 3 8 6 2 Serum creatinine (mg/dl) Urinary protein excretion (g/24 hours) 4 1 2 0 0 > 24 0 6 12 18 24 - 6 months
TYPE 2 DIABETES 200 Remission clinic SBP 180 160 Responder Non-Responder 140 (mmHg) 120 100 Responder 80 Non-Responder 60 40 > 24 0 6 12 18 24 - 6
Non-diabetic proteinuric nephropathies Diabetic nephropathy 25 25 25 20 20 15 15 13 Number Number 11 10 10 5 5 5 0 0 Non- responders Non- responders Responders Responders p < 0.01 non-diabetic proteinuric nephropathy vs diabetic nephropathy (Chi square test)
SWIMMING TO REDUCE PROTEINURIA? 20 patients: proteinuric chronic nephropathy Treatments: 12-week regular acquatic exercise Proteinuria Blood pressure p < 0.01 p = 0.005 1.5 150 140 1.0+0.3 130 120 mmHg g / 24h 1.0 0.5+.03 p < 0.05 100 90 80 0.5 70 Post Pre Post Pre Pechter et al., Nephrol Dial Transplant, 2003



![Prepare ACE-A1.2 Exam with Actual ACE-A1.2 Dumps [PDF]](https://cdn4.slideserve.com/7888335/arista-dt.jpg)
![Arista ACE-A1.2 Dumps - Actual ACE-A1.2 Questions PDF [Updated]](https://cdn4.slideserve.com/8039905/arista-dt.jpg)