Download
1 / 21
210 likes | 595 Views
February 24 – March 7, 2014. Claremore Indian Hospital BCMA (PSB 3*42) Deployment Site Visit. Background. Meaningful Use Stage 2 Criteria for Eligible Hospitals (EHs), and Critical Access Hospitals (CAHs):

E N D
February 24 – March 7, 2014 Claremore Indian Hospital BCMA (PSB 3*42) Deployment Site Visit
Background • Meaningful Use Stage 2 Criteria for Eligible Hospitals (EHs), and Critical Access Hospitals (CAHs): • Objective: Automatically track medications from order to administration using assistive technologies in conjunction with an electronic medication administration record (eMAR). • Measure: More than 10% of medication orders created by authorized providers of the EH or CAHs inpatient or emergency department during the EHR reporting period for which all doses are tracked using eMAR.
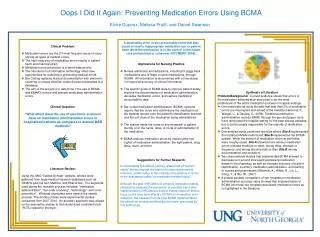
What is Bar Code Medication Administration (BCMA)? • BCMA is an Assistive Technology Software Application Developed and Used by the Veterans Health Administration (VHA) Facilities to Document Medication Administration Activities and Reduce Medication Errors • The VHA Bar Code Resource Office (BCRO) provides bar code verification services to IHS for wristbands and drug products that will not scan at the point of care and provide test results to the submitting facilities • The BCRO has Developed a Structured Process for Performing Usability Assessments of New Features to Assure Successful Adoption by End-Users • BCMA is a Component of the RPMS-EHR Certified Electronic Health Record
How is BCMA Used? • BCMA is an Integral Part of Patient Safety– Nurses Administer Unit Dose Medications, Including IV Piggyback Medications and IV Large-volume Medications, through BCMA • All Information is Documented with a Date/Time Stamp for Improved Accuracy of Clinical Information • The Documented Information is Available Throughout the Facility to Any Clinician as Part of the Patient’s Health Record • Pharmacy and Nursing Staff Must Collaborate Closely with Information Technology Services Staff if the Medication Administration Arm of the System is to Work Optimally
Claremore Indian Hospital BCMA Team • Jodi Tricinella, PharmD, Pharmacy BCMA Coordinator • Cindy O’Mary, ADN, RN, Nursing BCMA Coordinator • Cory Wilton, DPh, Pharmacy/Informaticist • Marty Smith, DPh, Clinical Applications Coordinator (CAC) • Tammy Wampler, BSN, RN, Chief Nurse Executive • Jim Smith, Information Technology Specialist • Jamie Rhodes, Patient Registration Director • Cindy Cates, Asst. Director, Health Information Management Systems (HIMS) • Peggy Shults, Director, Health Information Management Systems (HIMS) • Kelly Battese, PharmD, Ambulatory Care Director • David Ponder, Information Technology Director • Danna Roberts, ADN, BCMA Super User • Walter, DeLong, BSN, BCMA Super User • Michael Lee, PharmD, Pharmacy Director • Nancy Welch, Respiratory Therapy
Oklahoma Area BCMA Team • Amy Rubin, PharmD, CHTS-IS, MMI, Area Clinical Applications Coordinator (CAC), Area Meaningful Use Coordinator • Max Burchett, PharmD, Area Pharmacy Informaticist • Tracie Patten, PharmD, Area Pharmacy/Lab Consultant • Rebecca Loving, MS, RN Area Nurse Consultant • Robin Thompson, MS, APRN, CNS, Asst. Clinical Applications Coordinator (CAC) • Charles Cross, CMA, CSM, MCP, Area Information Technology Specialist • Jonathan Lambeth, Information Technology Specialist
VA Remote Cross Functional Team • Cathi Graves, Project Manager, BCRO, OIA, VHA • Kirk Fox, Clinical 1 Support Team, OIT, VA • Randall Baylis, BSBA, Clinical 1 Support Team, OIT, VA • Jonathan Bagby, MSN, MBA, RN-BC, Nurse Consultant, BCRO, OIA, VHA • Jan Zeller, MBA, BSN, RN, Education Project Manager, VA EES • Daphen Shum, BSPharm, RPh, Pharmacy Supervisor, Perry Point, MD, VAMC • Stephen Corma, BSPharm, RPh, Pharmacist Consultant, BCRO, OIA, VHA • Hugh Scott, MS, RNC, VHA Management & Program Analyst, Washington, DC, IHS/VHA Interagency Liaison • Barbara Connolly, Clinical 1 Support, OIT, VA
IHS On Site/Remote Cross Functional Team • David Taylor, MHS, RPh, PA-C, RN, BCMA Federal Lead, IHS/OIT • Deborah Alcorn, MSN, RN, CPC, BCMA Nurse Consultant, IHS/OIT • Phil Taylor, BA, RN, BCMA Nurse Consultant, MSC Contractor • Chris Saddler, RN, BCMA Information Technology Consultant, IHS/OIT via Remote Adobe Connect • Wil Darwin, National Pharmacy Council Chair • Northern Navajo Medical Center BCMA Team – Remote • Gallup Indian Medical Center BCMA Team – Remote • Chinle Comprehensive Health Care Center BCMA Team – Remote • Pine Ridge IHS Hospital BCMA Team – Remote
VA IHS BCMA Collaboration Effort • Includes BCMA Software, Hardware, and Medication Administration Process Reviews • FY13 – Implementation at 2 Indian Health Care facilities • FY14 – Implementation at 9 Indian Health Care facilities • FY15 – Implementation at 4 Indian Health Care facilities • VA IHS BCMA Cross Functional Team Kick-off March 19-21, 2013 • Remote Participation for Initial Configuration/Test/End-User Training-April 8-19, 2013, Albuquerque, NM • Ongoing Remote RPMS Pharmacy Drug File Cleanup – 6 week series • ADT delayed orders/auto DC of orders optimized to align with CMS 2 midnight rule and Interqual® criteria • Integrate ADT and BCMA implementation with the Baby Friendly Initiative including rooming-in
Configuration & Test Lessons Learned • Obstetrics/Newborn Wards and Beds Configured to Align with the Baby Friendly Hospital Initiative • Inpatient Medication for Outpatient (IMO) for Obstetric Triage • Wrist Band Printing • Increased Omnicell Time Interval to Allow for Medication Availability
Day Surgery • Used Observation Rules as a Guide for Configuration of Day Surgery to Facilitate Use of Delayed Orders, BCMA, and Safety during Transition of Care • Created Day Surgery Ward • Created New Day Surgery Specialty • Created New Day Surgery Treating Specialties • Configured ADT for New Day Surgery Ward • Programming Changes to Screen Day Surgery Patients from Inpatient Census Reports • BCMA Utilization Pre-op Medications will require additional Pharmacy Coverage
Training Activities • Friday – Training Preparation and Practice Session (10 Hours) • Sunday – Afternoon Super User Training Sessions (5 hours) • Monday – Morning and Afternoon Super User Training Sessions (4 hours Each) • Tuesday – Morning Super User Training Session (4 hours), Afternoon BCMA Pharmacy Training Session (4 hours), Evening Day Surgery Planning Session (3 hours) • Wednesday – Morning and Evening Super User Training (4 hours Each), Afternoon BCMA Coordinator/RN Finish Key Training (4 hours) • Go Live Wednesday Evening • Troubleshooting • Thursday – Debriefing, Go Live and Troubleshooting Continues Throughout Thursday and Friday Major Medication Passes (9:00 AM & 9:00 PM) 14 hours on Wednesday and 14 hours on Thursday • A Total of – 202 Training Encounters, of these 76 were Unduplicated Educational Encounters • Fifty percent (50%) Claremore Indian Hospital Pharmacy/ Nursing staff members who participated in the training will process/administer medications.
BCMA TrainingLessons Learned • Active engagement of House Supervisors and BCMA Coordinators is REQUIRED • Nursing Verification of Medication Orders in EHR • RN Finish Key Process and Order Verification Process in EHR must be carefully Understood and Delineated • Provide “At the Elbow” Support for Generating Reports (Due List, Missed Medication, PRN Effectiveness) Marking Medications and Adding Comments • Provide Orientation to WOWS, Battery Packs, Sign-ins
BCMA TrainingLessons Learned • Create Policies & Procedures to Align with New BCMA Processes: • Each Nurse to View Missed Med & PRN Effectiveness Reports at Specified Shift Intervals • Timely Medication Administration • Update Omnicell Medication Override Policy/Procedure • BCMA Competency Evaluation • Policy/Procedure for RN Finish Key and RN Order Verification in EHR • Accurate Medication Order Verification Process
Go LiveLessons Learned • Place Generic Log-on and Comment Scan Sheet on WOWS • Nursing to Use Due List to Obtain Medications from Omnicell • Nursing to Keep Virtual Due List Time Parameters Narrow • Each Nurse and Nurse Supervisor to View Missed Medications and PRN Effectiveness Reports at Specified Shift Intervals
Go LiveLessons Learned • ER Medications are on Paper Resulting in Difficult Medication Reconciliation with High Risk for Errors • BCMA Requires Real Time ADT • Incorporate BCMA Reports in Medication Error Review Committee and Root Cause Analysis Meetings and other PI activities • Claremore BCMA Team to Meet Weekly to Discuss Scanning Failures/Troubleshooting and Provide Feedback to All Clinical Staff
Post Implementation Statistics Wristbands Medications