Download
1 / 1
10 likes | 90 Views
Explore the correlation between substance abuse and opioid use in chronic low back pain patients. Learn about the risks and benefits of opioid therapy for pain management. Research findings suggest a need for balance to prevent abuse or diversion.

E N D
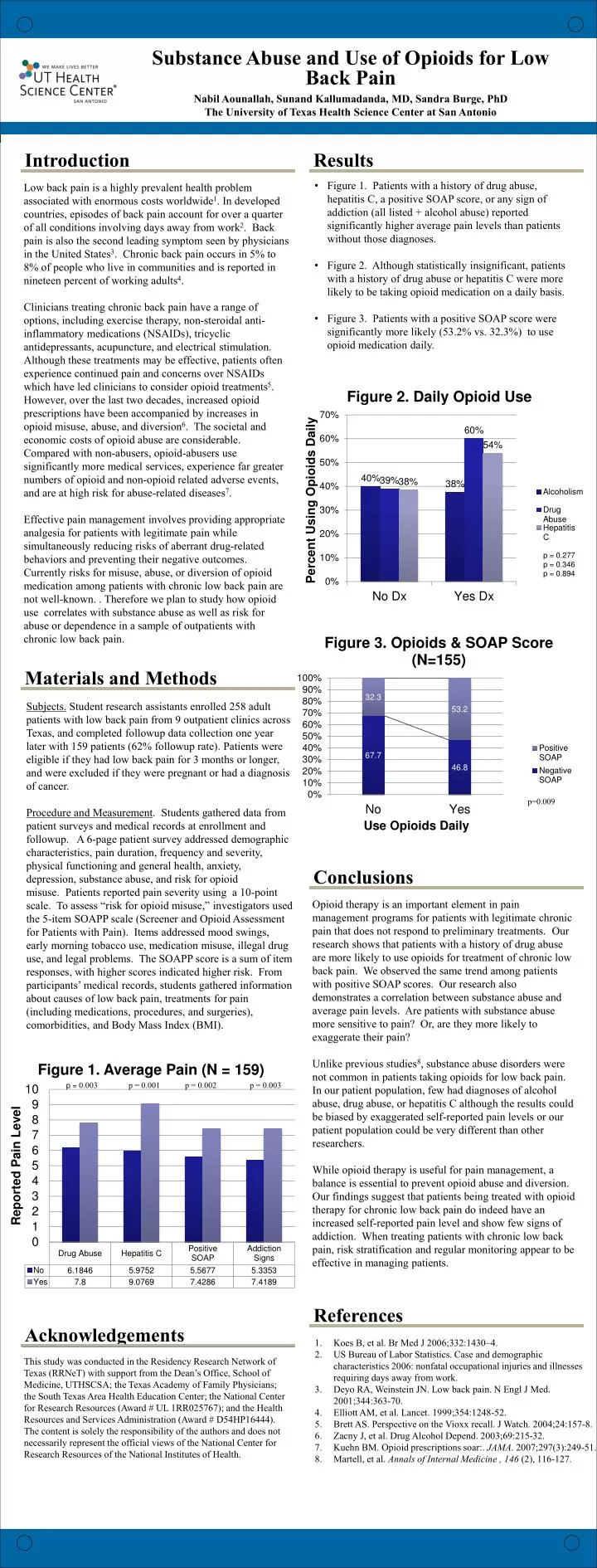
Substance Abuse and Use of Opioids for Low Back Pain Nabil Aounallah, Sunand Kallumadanda, MD, Sandra Burge, PhD The University of Texas Health Science Center at San Antonio Introduction Results • Figure 1. Patients with a history of drug abuse, hepatitis C, a positive SOAP score, or any sign of addiction (all listed + alcohol abuse) reported significantly higher average pain levels than patients without those diagnoses. • Figure 2. Although statistically insignificant, patients with a history of drug abuse or hepatitis C were more likely to be taking opioid medication on a daily basis. • Figure 3. Patients with a positive SOAP score were significantlymore likely (53.2% vs. 32.3%) to use opioid medication daily. Low back pain is a highly prevalent health problem associated with enormous costs worldwide1. In developed countries, episodes of back pain account for over a quarter of all conditions involving days away from work2. Back pain is also the second leading symptom seen by physicians in the United States3. Chronic back pain occurs in 5% to 8% of people who live in communities and is reported in nineteen percent of working adults4. Clinicians treating chronic back pain have a range of options, including exercise therapy, non-steroidal anti-inflammatory medications (NSAIDs), tricyclic antidepressants, acupuncture, and electrical stimulation. Although these treatments may be effective, patients often experience continued pain and concerns over NSAIDs which have led clinicians to consider opioid treatments5. However, over the last two decades, increased opioid prescriptions have been accompanied by increases in opioid misuse, abuse, and diversion6. The societal and economic costs of opioid abuse are considerable. Compared with non-abusers, opioid-abusers use significantly more medical services, experience far greater numbers of opioid and non-opioid related adverse events, and are at high risk for abuse-related diseases7. Effective pain management involves providing appropriate analgesia for patients with legitimate pain while simultaneously reducing risks of aberrant drug-related behaviors and preventing their negative outcomes. Currently risks for misuse, abuse, or diversion of opioid medication among patients with chronic low back pain are not well-known. . Therefore we plan to study how opioid use correlates with substance abuse as well as risk for abuse or dependence in a sample of outpatients with chronic low back pain. Materials and Methods Subjects. Student research assistants enrolled 258 adult patients with low back pain from 9 outpatient clinics across Texas, and completed followup data collection one year later with 159 patients (62% followup rate). Patients were eligible if they had low back pain for 3 months or longer, and were excluded if they were pregnant or had a diagnosis of cancer. Procedure and Measurement. Students gathered data from patient surveys and medical records at enrollment and followup. A 6-page patient survey addressed demographic characteristics, pain duration, frequency and severity, physical functioning and general health, anxiety, depression, substance abuse, and risk for opioid misuse. Patients reported pain severity using a 10-point scale. To assess “risk for opioid misuse,” investigators used the 5-item SOAPP scale (Screener and Opioid Assessment for Patients with Pain). Items addressed mood swings, early morning tobacco use, medication misuse, illegal drug use, and legal problems. The SOAPP score is a sum of item responses, with higher scores indicated higher risk. From participants’ medical records, students gathered information about causes of low back pain, treatments for pain (including medications, procedures, and surgeries), comorbidities, and Body Mass Index (BMI). Conclusions Opioid therapy is an important element in pain management programs for patients with legitimate chronic pain that does not respond to preliminary treatments. Our research shows that patients with a history of drug abuse are more likely to use opioids for treatment of chronic low back pain. We observed the same trend among patients with positive SOAP scores. Our research also demonstrates a correlation between substance abuse and average pain levels. Are patients with substance abuse more sensitive to pain? Or, are they more likely to exaggerate their pain? Unlike previous studies8, substance abuse disorders were not common in patients taking opioids for low back pain. In our patient population, few had diagnoses of alcohol abuse, drug abuse, or hepatitis C although the results could be biased by exaggerated self-reported pain levels or our patient population could be very different than other researchers. While opioid therapy is useful for pain management, a balance is essential to prevent opioid abuse and diversion. Our findings suggest that patients being treated with opioid therapy for chronic low back pain do indeed have an increased self-reported pain level and show few signs of addiction. When treating patients with chronic low back pain, risk stratification and regular monitoring appear to be effective in managing patients. References Acknowledgements Koes B, et al. Br Med J 2006;332:1430–4. US Bureau of Labor Statistics. Case and demographic characteristics 2006: nonfatal occupational injuries and illnesses requiring days away from work. Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344:363-70. Elliott AM, et al. Lancet. 1999;354:1248-52. Brett AS.Perspective on the Vioxx recall. J Watch. 2004;24:157-8. Zacny J, et al. Drug Alcohol Depend. 2003;69:215-32. Kuehn BM. Opioid prescriptions soar:. JAMA. 2007;297(3):249-51. Martell, et al. Annals of Internal Medicine, 146 (2), 116-127. This study was conducted in the Residency Research Network of Texas (RRNeT) with support from the Dean’s Office, School of Medicine, UTHSCSA; the Texas Academy of Family Physicians; the South Texas Area Health Education Center; the National Center for Research Resources (Award # UL 1RR025767); and the Health Resources and Services Administration (Award # D54HP16444). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources of the National Institutes of Health.






