Download
1 / 36
360 likes | 525 Views
Squamous Cell Carcinoma: An update on Treatment and Management. Ritu Saini, MD NY Medical Skin Solutions New York University Langone Medical Center. Epidemiology. 20% of all cutaneous cancers annually 200,000 new cases 30 00 deaths annually

E N D
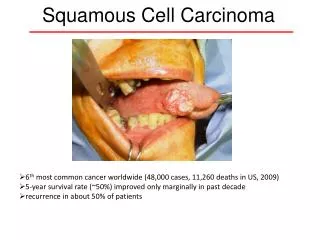
Squamous Cell Carcinoma:An update on Treatment and Management Ritu Saini, MD NY Medical Skin Solutions New York University Langone Medical Center
Epidemiology • 20% of all cutaneous cancers annually • 200,000 new cases 3000 deaths annually • Metastasis rate is 0.3-16% (mainly in high-risk SCC) • Lifetime risk • 14 % in Caucasian Males • 9% in Caucasian Females • Typical age of presentation age 70 highest incidence age 85 Holme SA et al. Br J Dermatol 2000; 143:1124-9 Veness MJ. Australian J Dermatol 2006; 47:28-33
Risk Factors for Squamous Cell Cancer • Sun Exposure (pre-cancerous actinic keratosis lesions) • Chronic Wounds • Marjolin’s ulcers (burn scars/decubitii) • Diabetes • Venous disease • Arterial insufficiency • Immunopathy (organ transplants ↑14 % scc:bcc 5:1) • Other malignancies • Wound healing complications following surgery *Commonly seen in geriatric population
Complete History and Physical • Etiology • Duration • Previous Treatment • History of similar wounds • Pain • History of skin cancer • Vascular • Neurological • Orthopedic
Treatment • Surgery • Standard exision • Mohs surgery • Electrodessication and curettage • Cryosurgery • Topical chemotherapies (Imiquimod, Fluorouracil) • Radiation • Systemic chemotherapies (largely reserved for OTR’s) * In elderly population greater potential for developing high-risk tumors Greater risk for metastasis
Features of High-risk SCC Jennings, L and Schmults, J Clin Aesthetic Dermatol. 2010;3(4):39–48.
Tumor Location • Arising in previously injured skin • Burn site • Scar • Chronic wound • Ulcer • Ear • Lip • Anogenital • Recurrence rate of 58% • Overall 5 year survival of 52% • *9 and 14% risk of metastasis, respectively compared to other sun exposed sites • 15-74% increased risk * Rowe DE et al. J Am Acad Dermatol. 1992;26(6):976–990.
Tumor Size • > 2 cm in size trunk and extremities • <2 cm in size • ≥ 1 cm – cheeks, forehead, scalp, neck ≥ 0.6 cm – “mask” or “H” area of face • Lip • Ear Higher recurrence (15% vs 7%) Metastatic rate(30% vs 9%) Review of 915 SCC risk of mets higher in tumors ≥ 1.5cm Prospective study of 266 patients with metastatic SCC, median size 1.5cm Moore BA et al. Laryngoscope. 2005; 115:1561-1567 Quaedvlig PJF et al. Histopathology. 2006
Courtesy of Head and Neck Brown University, Dermatologic Surgery Dept of Univ. of Washington, South Texas Skin Cancer Center, and Medscape
Histological Grade • 37% cure rate for poorly differentiated tumors • Desmoplastic (infiltrative) have high propensity for regional metastasis • 59% and 88% for moderately and well differentiated tumors, respectively • 22% vs 3.8% Lymph node metastasis • 27.4% vs. 2.6% local recurrence Mullen JT, et al. Ann Surg Oncol. 2006;13(7):902–909. Goepfert H, et al. Am J Surg. 1984;148(4):542–547.
Perineural Invasion • Occurs in 7% of cutaneous SCC • High incidence of recurrence, metastasis, and death • Outcomes are worse for those with clinical symptoms of perineural invasion. • Ross et al. reported poorer outcomes for those with involvement of nerves 0.1 mm or larger (32% increased risk of death) Ross AS, Whalen FM, Elenitsas R. Dermatol Surg. 2009;35(12):1859–1866.
Perineural Invasion Courtesy of Memorial Sloan Kettering
Staging • Regional Lymph node exam should be performed • Fine-needle aspiration or excisional biopsy for all enlarged nodes • + nodes should be resected • Adjuvant radiation 73 % five year survival
Sentinel Lymph Node Biopsy: Is it warranted in the staging of high-risk squamous cell carcinoma?
Sentinel Lymph Node Biopsy • Case reports and series – No controlled studies • Review of English literature • Anogenital and non-anogenital cases with clinically negative nodes analyzed separately • Percentage of (+) sentinel lymph node biopsy • False negative rates calculated • Local recurrence • Nodal and distant metastasis • Number of deaths from disease Ross AS, Schmults CD. DermatolSurg 2006; 32: 1309-1321
Review of English Literature (SNLB) Anogenital Non-anogenital • 607 patients • 24% +SNLB • False Negative rate of 4% • 85 patients • 21% +SNLB • False Negative rate of 5% Controlled studies are needed to demonstrate whether early detection of subclinical nodal metastasis will lead to improved disease-free or overall survival for patients with high-risk SCC SLNB accurately diagnoses subclinical lymph node metastasis with few false-negative results and low morbidity.
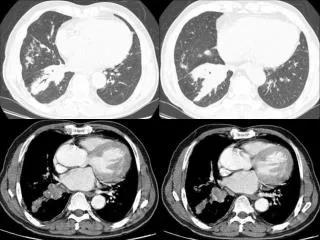
Imaging • Standard method to determine subnodal spread • Gold standard modality not well established in SCC • Can extrapolate using body of data from oro-nasopharyngeal tumors • Variable sensitivity and specificity for CT, MRI, PET • Survey study of 117 mohs surgeons • 35 % seldom image High-risk SCC patients • 54% - CT, 36% -MRI, 15%- PET
Imaging Computed Tomography Magnetic Resonance Imaging • Central nodal necrosis • Extracapsular Spread • Skull-based Invasion • Cartilage involvement • Neurotrophic tumors (advance perineural invasion) • Defines tissue planes • Distinguishes dense connective tissue from Muscle Imaging poses little risk and can be beneficial in preoperative planning and nodal staging if extensive tissue involvement is suspected
Treatment of high-risk SCC • Trunk and Extremities > 2cm (no other high risk factors) • Wide Excision with 1 cm margins • If margins negative • Follow up clinically • If margins positive • Mohs surgery for better margin control • Resection with complete circumferential peripheral and deep margin assessment with frozen or permanent sections
Treatment of High-risk SCC • Head and neck tumors with Palpable regional nodes or abnormal nodes on imaging • Perform Fine Needle Aspiration (FNA) • If FNA (-) • Re-evaluate clinically • Repeat FNA • Lymph node removal • If FNA (+) Head/neck Surgical consultation • Lymph node resection for surgical candidates • Adjuvant radiation therapy may be indicated • Radiation therapy for non-surgical candidates Practice Guidelines in Oncology – V.1. 2009 National Comprehensive Cancer Network (nccn.org
Adjuvant Radiation • Recommended for high-risk SCC especially in setting of perineural invasion • Review comparing high-risk SCC treated with surgery alone vs. surgery and adjuvant radiation therapy (ART) Jambusaria-Pahlajani A et al. Dermatol Surg. 2009;35(4):574–585.
Surgery vs. Surgery + ART • Primary outcomes assessed: • Local recurrences • Nodal Metastasis • Distant Metastasis • Disease-Specific Death • Methods/Subjects • No controlled studies found • 2449 cases of non-anogenital SCC • 2358 cases treated with surgery only • 91 cases treated with surgery and ART
Surgery vs. Surgery + ART • ART played the greatest role in cases of perineural invasion- with size of nerve being most important • <0.1 mm in diameter • Only 5% recurrence rate (n=1/22) • No metastasis • No disease-specific death • ≥ 0.1 mm in diameter • 50% risk of local recurrence • 38% risk of regional nodal metastasis • 32% distant metastasis with disease-specific death
Surgery vs. Surgery + ART • Surgery + ART • 19% regional metastasis • 13% distant metastasis • Surgery Alone • 10% regional metastasis • 4% distant metastasis • Data were not controlled for tumor stage • Likely more advanced disease • Clear surgical margins were not documented
Surgery vs. Surgery + ART • Clear Surgical Margins • 943 cases – clear surgical margins documented • 5% risk local recurrence • 5% regional mets • 1% distant mets • 1% disease specific death • Outcomes significantly better than in cases (1,506) when margin status not reported
Surgery vs. Surgery + ART • Conclusion • Cure rates are high when surgical margins are clear • It is not clear just which patients and to what extent they will benefit from adjuvant radiation therapy • May be indicated in certain situations • Named nerves or nerves > 0.1 mm • Uncertain or positive surgical margins • Inoperable cases • In-transit metastasis
Follow Up Local Disease Regional Disease • History and Physical • Q 3-6 months for 2 years • Q 6-12 months for 3 year • Annual exam for life • History and Physical • complete skin and regional lymph node exam • Q 1-3 months for 1 year • Q 2-4 months for 2nd year • Q 4-6 months for 3rd-5th year • Q6-12 months for life Patient education Sun avoidance Sunscreens Sun protective clothing Self skin examinations
Conclusions • Management of high-risk squamous cell carcinoma is complicated • Lack of prognostic and treatment guidelines make management nebulous • Best practice regimens based on retrospective studies • Controlled prospective studies needed for clarity
Conclusions • Early detection • Surgical treatments with clear margins when possible • Staging of draining nodal basins • Adjuvant radiation when indicated • Close follow up