Download
1 / 34
340 likes | 459 Views
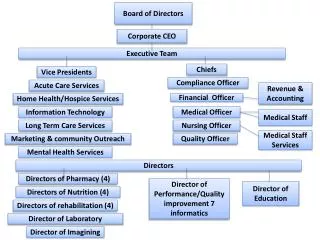
SustiNet Board of Directors. October 13, 2010 Anya Rader Wallack Katharine London Linda Green Stan Dorn. Recap of September 22 meeting. Discussion of delivery system reform and payment reform Draft recommendations sent to all board members

E N D
SustiNet Board of Directors October 13, 2010 Anya Rader Wallack Katharine London Linda Green Stan Dorn
Recap of September 22 meeting • Discussion of delivery system reform and payment reform • Draft recommendations sent to all board members • Some comments and additions received, others are welcomed (send to Anya: anya@arrowheadha.com) • Revised draft recommendations will be presented for your action at a future board meeting
Topic for today: governance and administration • How should SustiNet relate to current state agencies? • What are the ongoing roles and responsibilities of the SustiNet governing body? • To carry out these roles and responsibilities: • What governance structure is most appropriate? • What powers and duties are necessary? • What administrative structures and capacities are necessary? • Before 2014, should SustiNet be offered to small firms, municipalities, and non-profits? To individuals? • Starting in 2014, should SustiNet be offered in the Exchange?
Part I BACKGROUND
SustiNet law: role and governance • SustiNet is a self-insured health plan • SustiNet Health Partnership Board of Directors "shall offer recommendations to the General Assembly on the governance structure of the entity that is best suited to provide oversight and implementation of the SustiNet Plan" • Recommendations may include establishing a public authority • Long list of potential powers and duties that could be assigned to the authority, all associated with operating SustiNet
Federal health reform • The exchange serves • Small firms • Individuals without affordable access to comprehensive employer-sponsored insurance (ESI) • For eligible individuals and small firms, tax credits are available only through the Exchange • Qualified health plans must be • Offered by state licensed carriers • Available at silver and gold actuarial value levels
Health insurance carriers may offer: Where does SustiNet fit? Not a “health plan”: Self-insured plans or MEWAs (any plan that is exempt from state insurance regulation under section 514 of ERISA) [Sec. 1301(b)] Health plans Health insurance coverage and group health plans • Qualified health plans [Sec. 1301(a)] • Health plans that are • Certified by the Exchange (i.e. meet marketing req’s, network adequacy, accreditation, uses uniform enrollment form, etc.); [Sec. 1311(c) and (e)] • Provide essential health benefits; [Sec. 1302] and • Offered by a health insurance issuer that is licensed, offers at least one silver and one gold-tiered product, charges the same premium inside and outside the Exchange, and complies with any regulations established by DHHS. • Also includes CO-OPs, multistate plans, and qualified direct primary care medical home plans. Exchange-eligible plans
Part II OPTIONS FOR SUSTINET ROLE AND RELATIONSHIP TO STATE DEPARTMENTS AND THE EXCHANGE
SustiNet implements the country’s best thinking about how to slow cost growth while improving quality. Delivery and payment reforms include patient centered medical homes, HIT, realigned incentives, etc. Note: The SustiNet agency could handle all administration of the SustiNet plan in-house or it could contract with one or more third party administrators (TPAs) to carry out particular functions. DSS and Comptroller contract with SustiNet to provide coverage. What is SustiNet? Option A: SustiNet as health plan (Step 1 of 3) SustiNet governing body A B C D SustiNet Benefit Options DSS Comptroller Medicaid SEHP
What is SustiNet? Option A: SustiNet as health plan (Step 2 of 3) SustiNet governing body Individuals and small firms can buy SustiNet directly (beg. 2012) SustiNet A B C D E F SustiNet Benefit Options DSS Comptroller Medicaid SEHP
Individuals and small firms can buy SustiNet through the exchange (beginning 2014) What is SustiNet? Option A: SustiNet as health plan (Step 3 of 3) SustiNet governing body Exchange A B C D E F SustiNet Benefit Options DSS Comptroller Medicaid SEHP
What is SustiNet? Option B: SustiNet as overseer and health plan (Step 1 of 3) SustiNet governing body • Subject to federal law and collective bargaining agreements, SustiNet has ultimate responsibility for all DSS & Comptroller rules, regulations and procedures for Medicaid, SEHP, and other programs relating to: • delivery system requirements • performance improvement • provider payment methods & incentives • covered benefits • etc. DSS Comptroller Medicaid SEHP A B C D SustiNet Benefit Options
What is SustiNet? Option B: SustiNet as overseer and health plan (Step 2 of 3) SustiNet governing body Individuals & Small Businesses can purchase SustiNet directly (beg. 2012) DSS Comptroller Medicaid SEHP A B C D F E SustiNet Benefit Options
What is SustiNet? Option B: SustiNet as overseer and health plan (Step 3 of 3) Individuals & Small Firms can buy SustiNet through Exchange (beg. 2014) SustiNet governing body DSS Comptroller Medicaid SEHP Exchange A B C D F E SustiNet Benefit Options
What is SustiNet? Option C: SustiNet as consolidated agency and health plan (Step 1 of 3) Authority for administering the Medicaid, SEHP and other programs is transferred from DSS and the Comptroller to a new entity, with a policy-setting governing body (consistent with federal law and collective bargaining agreements). SustiNet Governing Body SustiNet Medicaid SEHP
What is SustiNet? Option C: SustiNet as consolidated agency and health plan (Step 2 of 3) SustiNet Governing Body Individuals & Small Businesses can purchase SustiNet directly (beginning 2012) SustiNet Medicaid SEHP Commercial-style benefits
What is SustiNet? Option C: SustiNet as consolidated agency and health plan (Step 3 of 3) SustiNet Governing Body Exchange SustiNet Medicaid SEHP Commercial-style benefits Individuals & Small Businesses can buy SustiNet through the Exchange (beginning 2014)
Discussion: some considerations for choosing among these options • Who has ultimate decision-making authority? • Who controls funding? • What are the administrative expenses associated with the model, for the state, individuals, and firms? • Does the model facilitate efficient and effective program management? • How would the model facilitate coordination across programs/conflict resolution? • What approvals are necessary (e.g., Medicaid waiver)? Are there other barriers to implementation? • What are the issues and costs related to program alignment/realignment/transition?
Other key issues: which entity has legal authority & responsibility for • Serving as single state agency, for purposes of Medicaid and CHIP (including CMS relations, eligibility, enrollment, appeals, etc.)? • Promulgating & enforcing rules and regulations? • Allocating funding across eligible populations & programs? • Negotiating and enforcing collective bargaining agreements with state employees?
Why offer SustiNet outside the exchange in 2014 and beyond? • Firms with >100 full-time employees • Can’t use exchange till 2017 • For firms large enough to be self-insured, may be easier to prevent adverse selection outside the exchange • Small firms • For 2 years, firm tax credits limited to exchange • Exchange requires list billing. Outside the exchange, firms can group bill. • Undocumented immigrants can’t buy individual coverage in the exchange
Part III SUSTINET GOVERNANCE
Additional governance issues • What is the size and makeup of the governing body? • How are individuals selected? • What disciplines should be represented? • What decision-making authority does the governing body have? • What rules and procedures apply to their decisions? • What advisory bodies will be established?
Advisory Committee recommendations: Governance and Administration SustiNet Board should: • Include at least 2 enrollees in the SustiNet plan • Reflect the diversity of SustiNet plan members • Include at least 2 individuals who have experience in reducing health disparities SustiNet Board should establish formal relationships with: • CT health agencies (e.g. DSS, DPH, DMHAS, DCF) • Health Information Technology Exchange of Connecticut (HITECT) • Related federal councils and task forces
Advisory Committee recommendations: Governance and Administration Establish independent statewide councils • Patient Centered Medical Home • Obesity Establish Board committees • Health care quality and payment • Health care safety • Preventive health care • Community advisory • Health disparities and equity
Part IV SUSTINET ADMINISTRATIVE NEEDS
Necessary administrative capacities for SustiNet, regardless of model chosen • Eligibility determination and subsidy calculations • Enrollment into plans • Premium billing/collection • Marketing (if offered to new populations) • Provider contracting and payments • Customer relations • Quality and safety standards • Data exchange • Utilization management • System management to achieve measurable objectives re disparities, chronic illness, etc.
Decision points On governance: • Preferred model for SustiNet role and structure? • Nature and composition of governing entity? • Decision-making authority? On administration: • Build versus buy? • Use existing state Medicaid or SEHP capacity? • How to achieve efficiencies? On access to SustiNet: • Before 2014, offer SustiNet as an option to small firms, municipalities, non-profits? To individuals? If so, how to prevent adverse selection? • Starting in 2014, offer SustiNet in the exchange?
Work plan for the next two months • November: costs and financing (includes implications of pursuing the federal Basic Health Program option) • December: two meetings: wrap up deliberations, and review draft report
Appendix A SUSTINET INFORMATION TECHNOLOGY, DATA AND EVALUATION NEEDS
SustiNet information technology needs • Eligibility determinations • Enrollment process and maintaining records • Premium billing, collection and related accounting functions • Payment for services • Annual reconciliations (e.g. performance incentives, PCMH-specific annual payments) • Provider network management • Evaluation data • Consumer-facing website
Guidance from Advisory Committees and Task Forces about Data Needs • Capture race and ethnicity data • Support care coordination across multiple provider settings • Capture HEDIS measures • Baseline utilization measurement • PCMH evaluation should be broad (e.g. transition planning) and deep (e.g. completeness of wellness visits). Should include qualitative measures as well. • Data collection strategies should minimize administrative burden on providers
Potential recommendations regarding SustiNet information technology • Plan for a multi-year phase in and consolidation • Identify capacity within existing state systems to add on Sustinet enrollment, eligibility and premium handling functions • Assess current information exchanges between DSS and OCA and health plans to identify options for Sustinet • Create Sustinet-specific finance and accounting structure, including payment, contract reconciliation and rate setting capacity • Data and analytics should be driven by a set of reporting principles and priorities. • Options for managing data and analytics include: • Standardized reports provided by all carriers (including Medicaid fee for service) • SustiNet plan-specific standardized reports provided by a TPA or MCO • Datasets provided by TPA or MCO and analyzed by SustiNet or an analytic contractor
Appendix b FOLLOW-UP ON POTENTIAL SUSTINET POPULATIONS