Download
1 / 33
330 likes | 346 Views
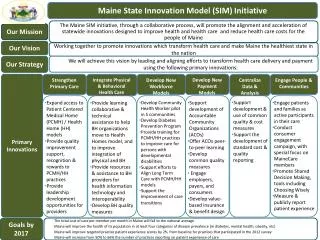
Review of MaineCare's progress through SIM objectives, including Behavioral Health Homes, Workforce Development, and Consumer Interviews. Analysis of cost findings, core metrics trends, provider and stakeholder feedback.

E N D
Maine SIM Evaluation Subcommittee September 2015 September 23, 2015
Welcome, Introductions, and Goals for Today’s Meeting • Review learnings to date and discuss opportunities for Rapid Cycle Improvement (RCI); • Discuss status of Medicare & Commercial Target setting process • Review current status of the Dashboard of Core Metrics • Receive a progress report of separate evaluations conducted by JSI on NDPP & CHW programs
Meeting Minutes Please see meeting minute handouts for August 26th • Suggested edits from Committee members? • Additional questions or clarifications? • Motion to approve as written or amended
Rapid Cycle Improvement (RCI) Discussion Preliminary data related to Provider / Stakeholder/ Consumer interviews and claims-based data compiled for the Maine Leadership Team (MLT) & the Strategic Objective Review Committee (SORT) to begin to explore answers to the following questions • What are the early impacts of SIM? • How is the implementation process going? • How can we improve it?
MaineCare SIM Objectives: MC1- Accountable Communities AC’s: • AC’s implemented in August 2014 therefore too soon to report conclusive quantitative claims-based analysis of their impact on health outcomes. • In general, consumers attributed to ACs rated patient-provider communication highly; however, this appears to be the case when the communication is unidirectional – i.e., the provider is communicating with the patient. Patients rated providers lower in their ability to listen to and engage their patients MC2- Behavioral Health Homes/Stage B Health Homes (see next slide) MC 3- Health Homes Workforce Development: Plan for workforce development has been completed; implementation pending. MC4- Intellectual/Developmental Disabilities (I/DD) Training for PCPs: PCP training has been initiated for this objective and more training sessions are planned. Stage A Health Homes not a SIM objective, but has integral role in the overarching SIM goals & multiple objectives therefore included in this report. (see subsequent slide)
MaineCare MC2- Behavioral Health Homes / Stage B Health Homes(page 1 of 3) Cost Findings: • Costs were $150 per member per month (PMPM) lower than for the control group. • Lower total costs for BHH consumers were driven by: • Lower professional behavioral health and case management expenditures. • Reduced expenditures on autism & child psychoses, attention deficit disorder, and anxiety disorder/phobia. Core Metrics Trends: • Follow-up after Hospitalization for Mental Illness increased more rapidly from 2013 to 2014 (up 52.1%) than from between 2012 to 2013 (0.2%). • Non-emergent emergency department admissions declined more rapidly between 2013 and 2014 (9.8%) than from between 2012 to 2013 (8.1%). • Median fragmented care index decreased between 2013 and 2014 (3.9%), similar to the decrease in overall MaineCare consumers (3.3%) during this same time. • Access to primary care for children aged 7 to 11 increased between 2013 and 2014 (6.7%), while overall MaineCare consumers trended downward (2.8%) • For both BHH and overall MaineCare consumers, Diabetic HbA1c tests trended in a negative direction; this was more pronounced for BHH consumers (13%) between 2013 and 2014 than overall MaineCare consumers (10.8%)
MaineCare MC2- Behavioral Health Homes / Stage B Health Homes(page 2 of 3) Provider / Stakeholder Interview Findings: • 20 of 34 (48%) of respondents stated that the BHH program has led to somewhat more patient engagement; 14 of these (33%) much more patient engagement. • 13 of 15 (87%) made positive comments about active changes the initiative had assisted them in making, including 11 who noted improvements in integrated care or patient care coordination • 18 of 32 practices commented about the effectiveness of BHHs on specific subgroups of patients: • 8 reported that “high need”/chronic patients tend to benefit more • 3 said patients living in rural areas were more difficult to engage • 13 of 16 (81%) BHH practices who expressed opinions about the PMPM (case rate), questioned its sustainability (i.e., whether it was sufficient)
MaineCare MC2- Behavioral Health Homes / Stage B Health Homes(page 3 of 3) Consumer Interview Findings: Compared with the control group, the intervention group rated: • Cultural sensitivity, participation in treatment planning, and quality and appropriateness of care more positively. • Social connectedness and outcomes less positively. 33% strongly agreed that (except for their current service providers) in a crisis they would have the support they need from family or friends. • Outcomes and Functioning • 22% of respondents strongly agreed that their symptoms are not bothering them as much, due to the impact of their services. • 29% of consumers strongly agreed that they or their child was better able to handle things when they went wrong. *Domains are composed of multiple items, and to calculate a score, all individuals responding to 50% or more items within the domain are assessed. The percentage presented represents individuals responding with the two most positive responses available in each item averaged across the number of items they answered within the domain.
MaineCare Stage A Health Homes (HH’s) (page 1 of 2) Cost Findings: • Stage A Health Homes members costs were $110 PMPM lower than the control. Expenditures also remained lower than the control group throughout 2014. Savings were driven by lower than expected expenditures the following areas: • Community Care Teams (CCT) hadhigherexpenditures than the control group Core Metrics Trends: • The median Fragmented Care Index decreased (0.9%), and the percent of members who did not have an imaging study for low back pain increased (up 2%) between 2012 and 2013 (positive finding). • Well-Child Visits for children ages 3 to 6 increased (up 10.8%), higher than the overall MaineCare members trend (up 3.8%) • Developmental screenings in the first three years of life also trended upwards (67.6%), while the overall MaineCare members trended upwards at a higher rate (100%)
MaineCare Stage A Health Homes (HH’s) (page 2 of 2) Provider / Stakeholder Interview Findings: • Of 85 providers and stakeholders who commented about primary care, 33 (39%) recommended more flexible attestation, reporting, reimbursement policies. • 29 out of 50 (58%) of practices made positive commentsabout the effectiveness of CCTs, including positive impacts on patient care or integration with the HHs • 64 of 69 (93%) of providers from HHs, BHHs, and CCTs mentioned that they use the HHES portal to some degree and it is used as a reimbursement tool Consumer Interview Findings: • 50% indicated their provider’s office talked with them about a personal problem, family problem, alcohol use, or a mental illness. • 38% reported that their provider’s office talked about their child’s learning ability. • 40% reported someone in their provider’s office asked them if there were things that made it hard to take care of their own or child’s health. • Relative to the control group, people rated HHs: • More positively on provider attention to mental and emotional health; • Less positively for follow-up on test results, provider advice on keeping children safe and healthy, and provider attention to a child’s growth/ development
Quality Counts (QC) SIM Objectives: QC1- Learning Collaborative for Health Homes (see next slide) QC3- Learning Collaborative for Behavioral Health Homes (see subsequent slides) QC 4- Quality Improvement Support for Patient-Provider Partnerships Pilots (P3 Pilots) : • Pilot completed in March 2015- 10 provider practices actively participated • Provider participation in P3 Learning Collaborative exceeded targets • Consumer interview questions have not been analyzed specific to this objective. Please refer to consumer interview findings for Stage A Health Homes for analysis regarding consumer engagement experience overall.
Quality Counts– QC1 Learning Collaborative for Stage A Health Homes • 40 of 44 (91%) HH providers provided positive comments about Quality Counts Learning Collaboratives sessions. • Providers suggested advanced topics and structured peer-facilitated learning opportunities. • Consumers highlighted the need for providers to solicit more information from consumers and further engage them in their own care – topics that could be addressed in future Learning Collaboratives. • Specific topics for which positive comments were received include:
Quality Counts– QC2 Learning Collaborative for Behavioral Health Homes • 91% of Behavioral Health Homes interview respondents made positive comments about the Learning Collaborative sessions facilitated by Quality Counts with half noting the value of networking and peer supports. • In addition, consumer feedback described under the Stage A HH objectives can help inform this objective. Given that a minority of consumers felt that the services helped improve their situation, future Learning Collaborative sessions might focus on ways to improve treatment efficacy and strategies for improving consumer engagement in treatment.
Center for Disease Control (CDC) SIM Objectives CDC1- National Diabetes Prevention Program (NDPP)**: • Preliminary findings indicate that providers participating in the program perceive it favorably, and respondents have recommended that this model of engagement could be used more broadly. CDC2-Community Health Worker (CHW Pilot)**: • 5 out of 61 provider interview respondents said they used CHW services. (This is not surprising given the small size of the program, the limited number of participating providers, and the recent program implementation as related to the timing of the provider surveys.) **Additional findings for CDC1 and CDC2 will be available through an evaluation being conducted by John Snow, Inc. (JSI).
Health InfoNet (HIN) SIM Objectives (page 1 of 2) HIN1- Notifications of Emergency Department Utilization for MaineCare: • Preliminary interview findings suggest that ED notifications have successfully engaged providers;. • Activities to further disseminate and strengthen regular use of this resource among providers may prove beneficial. • Given the number of electronic data portals and data sources currently deployed in Maine, Lewin is further vetting provider/stakeholder interview findings relating to this Objective to identify other potentially relevant findings for inclusion in the first Annual Evaluation Report. HIN2- Incentives for Electronic Health Record: • Twenty organizations are participating in the program; • Reimbursements are affected by the number of organizations who have met the initial milestones to enable them to receive funding.
Health InfoNet (HIN) SIM Objectives (page 2 of 2) HIN3- Connect Behavioral Health organizations to the Health Information Exchange (HIE): • While the number behavioral health sites connected to the HIE exceeded the original targets, the program has not met targets to establish bidirectional connections to the HIE. • A small numbers of providers (5) volunteered that interconnectivity between EMRs and the HIE was “challenging”, suggesting that more support may be needed. HIN also acknowledged this issue in their most recent quarterly report FFY2 Q3. HIN4- Provider Dashboard: • This objective will move into a testing phase in mid-September 2015. Further information and analysis of the Dashboard’s impacts will be provided in later reports. HIN5- Patient Portal: • The “Blue Button” initial pilot program was completed by June 2015- the SIM consumer survey did not include questions related to the patient portal.
Maine Health Management Coalition (MHMC) SIM Objectives (page 1 of 3) MHMC1-Track Health Care Costs: No preliminary / material data available to Lewin for analysis. Lewin is further vetting provider/stakeholder interview data to identify other potentially relevant findings for inclusion in the first Annual Evaluation Report. MHMC2- Value Based Insurance Design: • Preliminary interview findings indicate that 24 out of 44 (55%) of provider respondents noted they were affected by VBID; however, of these, 4 felt the changes were negative (e.g. staffing cuts or less time with the patients and more time with administrative tasks). These responses raise questions about the visibility of VBID and the need to consider ways to streamline administrative requirements. • Lewin is further vetting provider/stakeholder interview data to identify other potentially relevant findings for inclusion in the first Annual Evaluation Report.
Maine Health Management Coalition (MHMC) SIM Objectives (page 2 of 3) MHMC3-Public Reporting for QI and Payment Reform: • As of FFY2 Q3 ending June 2015, the goal for the percentage of Maine residents covered by alternative payment arrangements was exceeded. • The provider survey did not ask specifically about QI and Payment Reform objective; however, 19 providers expressed concern about the administrative burdens associated with payment reform, attestation, and healthcare reform more generally. MHMC4- PCP Access to Provider Portals: The number of practices (290) that have adopted claims portals exceeded the goal of 275. Further analysis of data available to Lewin will occur and be included in the Annual Evaluation Report.
Maine Health Management Coalition (MHMC) SIM Objectives (page 3 of 3) MHMC5- Practice Reports: • The total percentage of primary care practices receiving practice reports was exceeded for FFY2 Q3 ending June 2015. • Some HH interview respondents noted positive changes, such as the ability to drill down to the patient level data and to see how well the practice compares on various measures. • Other providers interviewed stated that the reports had limited impact on their practice, noting that the data is not useful because it is outdated. MHMC6-Consumer Engagement: • Quarterly reports ending June 2015 indicate lower consumer participation rates than planned, however MHMC completed a variety of stakeholder engagement sessions during that quarter. • As related to the “Get Better Maine” website, while 37 of 77 provider interview respondents were aware of the website, opinions were divided about its value. • Greater promotion of "Get Better Maine” and training resources that support consumers in their use of this data may lead to increased use of the website as part of provider quality improvement activities.
Commercial Target setting update • OCQI/SIM Project Director & Lewin met with K. Pelletreau & representatives from the health plans on September 10 • Reviewed purpose of target setting • Explained high-level process for development of MaineCare targets • Clarified Lewin’s role to provide technical assistance, not to set targets • Data sources reviewed; exclusions being vetted with MHMC • Next steps • Lewin to provide draft available baseline commercial SIM Core Metric data to health plan leaders & further vet to assure accuracy • Review technical details of target setting methods used for MaineCare targets • Review latest iteration of dashboard design with health plan representatives • Develop targets & related communication plan
Maine SIM Core Metrics dashboard updates • MaineCare • Commercial • Medicare
Evaluation Updates - CHW & NDPP • Evaluation components being conducted by John Snow Inc. (JSI) • CHWI Evaluation objectives: • Evaluation of four CHW Pilot Projects: project steps, tasks, barriers, solutions, and successes. • Capacity-Building Evaluation of CHW Initiative: assess sustainable capacity to support CHWs in Maine (CHW and supervisor training, hiring, and recommendations for future infrastructure.) • NDPP Evaluation objectives • Process evaluation that captures projects steps, tasks, barriers, solutions, and successes through the project period (October 2013 – September 2016). • Formative evaluation to document and support learning and information from the partners/organizations engaged throughout the project period. The formative evaluation will guide strategy development for payment test for SIM Years 2 & 3. • Using RE-AIM Framework • Reach, Efficacy, Adoption, Implementation, Maintenance
Evaluation Updates - CHW & NDPP (continued) • Activities since last update - CHWI Evaluation • Research Questions Defined – Stakeholder Workgroup • To what extent are model components implemented consistently and with fidelity? • What factors are associated with patient engagement and satisfaction in CHW services? • What resources are needed (both for local CHW model implementation and for the statewide system to support the model) to ensure consistent and effective implementation? • Data Collection • Grantee reports • Key informant interviews • CHW log/encounter forms • Patient satisfaction surveys
Evaluation Updates - CHW & NDPP (continued) • Activities since last update - NDPP Evaluation • Research Questions Defined – Stakeholder Workgroup • What systems, practice and beneficiary level factors are associated with a sustainable NDPP program? • What was the reach of NDPP? • Data Collection • NDPP aggregate participant data • Key informant interviews • Lifestyle coach survey
Next Steps • Change of Meeting dates beginning December 2015 • Any new risks identified?? • Next Meeting • October 28, 2015, 3-5 pm Conference room A 35 Anthony Avenue, Augusta • Future Discussion Topics • Continued RCI discussion & data analysis • Target setting progress for Commercial & Medicare • Refinements to interview tools for next round of interviews • Sustainable Research Collaborative • Follow up on identified risks as necessary