Download
1 / 27
270 likes | 348 Views
Volume of alcohol consumption, patterns of drinking and burden of disease in the Americas 2002. Jürgen Rehm 1,2,3 & Benjamin Taylor 2 1 Institut für Suchtforschung (ISF - Addiction Research Institute), Zurich, Switzerland 2 Centre for Addiction and Mental Health (CAMH), Toronto, Canada

E N D
Volume of alcohol consumption, patterns of drinking and burden of disease in the Americas 2002 Jürgen Rehm 1,2,3 & Benjamin Taylor 2 1 Institut für Suchtforschung (ISF - Addiction Research Institute), Zurich, Switzerland 2 Centre for Addiction and Mental Health (CAMH), Toronto, Canada 3 University of Toronto, Canada
Causal model of alcohol consumption, intermediate mechanisms, and long-term consequences * Independent of intoxication or dependence
Adult per capita consumption inlitre pure alcohol 2000 (based on CRA)
Estimation of AAF for different disease categories Volume of drinking Drinking pattern hazard score (predominance of intoxication) Other chronic Diseases (except CHD and depression) Injuries Coronary heart disease Alcohol- attributable conditions (by definition) Depression from psychiatric surveys
Alcohol related disease and injury • Chronic disease: • Cancer: Mouth & oropharyngeal cancer, Esophageal cancer, Liver cancer, Female breast cancer, other neoplasms • Neuropsychiatric diseases: Alcohol use disorders, unipolar major depression, epilepsy • Diabetes • Cardiovascular diseases: Hypertensive diseases, ischemic heart disease, stroke • Gastrointestinal diseases: Liver cirrhosis • Conditions arising during perinatal period: Low birth weight • Injury: • Unintentional injury: Motor vehicle accidents, drownings, falls, poisonings, other unintentional injuries • Intentional injury: Self-inflicted injuries, homicide, other intentional injuries
Classification of countries in WHO European regions by childhood and adult mortality (WHO, 2000) Definition of regions*: The regional subgroupings used were defined by WHO (World Health Report 2000) on the basis of high, medium or low levels of adult and of infant mortality.
Estimates of alcohol-related burden in South America • Epidemiological developments (i.e. changes in distribution of disease such as chronic disease vs. infectious disease) • Changes in drinking (average level and patterns of drinking) => slides with green background
Exposure: Characteristics of adult alcohol consumption in different regions of WHO AMRO:based on CRA 2000 (i.e. no new data on consumption included)(population weighted averages across countries; cf. Rehm et al., 2003b, 2004; Babor et al., 2003)
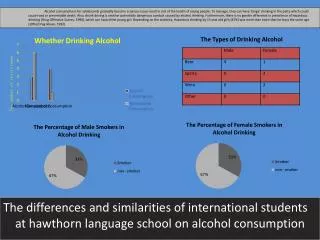
Adult alcohol consumption in different categories 2000 in % - Americas - males
Adult alcohol consumption in different categories 2000 in % - Americas - females
And after GENACIS and World Health Surveys and new per capita estimates (2002)….? • Similar overall consumption rates • Different distributions between ages • Different distributions between drinking categories:=> Higher proportions of people with heavy drinking
Changes between 2000 and 2002 estimates in different categories of alcohol consumption females males
Alcohol-attributable deaths in Americas 2002 by disease and region – epidemiological model
Alcohol-attributable mortality 2002 (number of deaths) – America epidemiological model vs. world
Comparison of alcohol-related deaths of 2002 to 2000 – epidemiological model only • For all of America, the relative size of mortality of alcohol-related deaths decreased slightly (4.4% in 2002; 4.7% in 2000). • The numbers of alcohol-related deaths -decreased in all three regions, with biggest decreases in America Region D. • For the world, the relative size of alcohol-related deaths stayed at about the same level (3.2% in 2000; 3.1% in 2002).
Alcohol-attributable deaths 2002 (basis: new alcohol prevalence estimates and epidemiological shifts in COD)
Comparison chart on alcohol-attributable deaths: best estimates 2002 versus 2000 estimates
Comparison of alcohol-related deaths from 2000 to 2002 – best estimates for 2002 • There are no major changes in estimates of alcohol-related mortality from 2000 to 2002 • Two developments: • Epidemiological change -> less deaths in alcohol-related categories • More heavy drinking -> more deaths…. • Americas continue to have a high mortality burden from alcohol • Please note, that this is a net burden, after subtracting cardio-protective effects
Alcohol-attributable BOD in DALYs 2002 (basis: new alcohol prevalence estimates and epidemiological shifts in COD)
Comparison chart on alcohol-attributable DALYs: best estimates 2002 versus 2000 estimates
Comparison of alcohol-related DALYs from 2000 to 2002 – best estimates for 2002 • There are no major changes in estimates of alcohol-related burden of disease from 2000 to 2002 • Americas continue to have a burden of disease from alcohol • Please note, that this is a net burden, after subtracting cardio-protective effects
Relative impact of alcohol for different age groups • For all three regions, for both genders, with one small exception, the relative weight of alcohol on deaths is strongest in the age group 15-29 years of age • In this age group, there are no beneficial effects of alcohol on mortality
Age and sex distribution among alcohol-related deaths in WHO America regions and in World for the year 2002 (own calculations)
Conclusion for policy -> main targets based on epidemiology This is the major aim of this conference, but from an epidemiological side, policies to reduce health burden in the following areas should be considered: • Heavy drinking occasions • Overall level of consumption • Youth • Injury • Alcohol use disorders