Download
1 / 30
300 likes | 494 Views
A NEEDS-BASED ANALYTICAL FRAMEWORK FOR HEALTH HUMAN RESOURCES PLANNING. Centre for Health Economics and Policy Analysis, (CHEPA) McMaster University Hamilton Health Economics Research at Manchester (HERMAN) University of Manchester, UK

E N D
A NEEDS-BASED ANALYTICAL FRAMEWORK FOR HEALTH HUMAN RESOURCES PLANNING • Centre for Health Economics and Policy Analysis, (CHEPA) McMaster University Hamilton • Health Economics Research at Manchester (HERMAN) • University of Manchester, UK • Centre for Health Economics Research and Evaluation (CHERE) • University of Technology, Sydney • Health Economics Unit, University of Cape Town, SA Stephen Birch
HEALTH HUMAN RESOURCES PLANNING: Focus: Impact of demographic change Effect of aging population on the provider requirements Effect of aging workforce on capacity to meet requirements General approach: Provider-population ratios applied to population projections (possibly with age and sex adjustments) Estimate shortfalls/surpluses in providers and calculate changes in the size of training programmes required to eliminate imbalances “How many additional physicians do we need to train?”
HEALTH HUMAN RESOURCES PLANNING: • Performed in isolation of other aspects of health care policy and population health • Research questions implicit, unclear or poorly defined • “How many health care providers are required to . . . serve future populations in the same way as the current population is served?” • Requirements determined by factors beyond control of policy • Underlying assumptions: • Population age structure determines service requirements (i.e., epidemiology constant) • Provider age structure determines the quantity of care provided (i.e., production function constant)
EXAMPLE: HHRP FOR DENTISTS IN UK (Birch and Maynard 1985) Method: Project ‘service use-population’ ratios onto expected future population Requirements: Assumed needs by age group constant Ignores impact of diet, oral hygiene, fluoride Supply: Assumed services per provider constant Ignores impact of technology (multi chairs, hygenists) Outcome: No evidence of excess supply Orthodontics (‘service deepening’ or ‘supplier induced demand’)
EXAMPLE: HHRP FOR PHYSICIANS IN CANADA • Royal Commission – Maintain pop-phys ratio(PPR) at 850 • Increase med. school intake for expected population growth • 1991 Barer-Stoddart report - PPR fallen rapidly – population growth less than projected • Stabilise PPR at 500-550 through package of measures including reductions in med school intake • 1998 Canadian Medical Association (CMA) population growth exceeded physician growth over post 91 period – 5 less docs per 100,000 (PPR growth 2.6% or less than 0.5% per year) • CMA estimated physician-population ratio to fall by 31% over 25 years - medical school intake increased
EXAMPLE: HHRP FOR PHYSICIANS IN CANADA Applying 1% annual reduction in needs and 1% annual increase in productivity to CMA estimates produces reduction of 27% in ‘effective’ PPR over same period (Birch et al. 2007) 2004 PPR = 471 much less than previous targets CMA acknowledge overestimated population growth and physician retirements so potential shortages inflated Any changes in productivity or needs would further reduce shortages or produce surplus Between 1961 and 2003 63% increase in physicians after allowing for population growth
IMPLICATIONS OF TRADITIONAL MODEL PEADIATRICIANS IN US 2004 Shipman et al. Numbers of pediatricians and children in US increase by 64% and 9% respectively by 2020 To maintain workloads need to ‘expand services and expand patient populations beyond current age groups’ 2008 American Academy of Pediatrics: Recommendations for cholesterol screening and treatment for children age 2 and over
AN EARLY DIAGNOSIS? “Progress in medicine does not focus on doing existing things more cheaply and simply, but on discovering complex and difficult things to do that previously could not be done at all . . . . . .the NHS was a miscalculation of sublime dimensions” Enoch Powell, Minister for Health, (1962)
CONCEPTUAL FRAMEWORK HHRP occurs within, not independent of, health care planning Health care planning occurs within, not independent of, public policy planning. HHRP incorporates dynamic and interacting nature of factors previously conceptualized as constant and independent.
FEATURES OF CONCEPTUAL FRAMEWORK Evidence-based approaches to needs: Need independent of availability or use ‘Derived’ nature of requirements: Requirements derived from the need for services Production of health care: Services produced from human and non-human resources. Contextual nature of requirements: Service contexts define opportunities and constraints for HHRP Range of policy levers: Training seats just one of many policy levers
ANALYTICAL FRAMEWORK: Two independent components: Provider supply How many providers are (or will be) available to deliver health care services to the population? Provider requirements How many providers are required to ensure sufficient ‘flow’ of health care services to meet the needs of the population?
DETERMINANTS OF PROVIDER SUPPLY Stock of individuals M Number of providers potentially available to contribute to service production Flow of activities, Ls generated from the stock Quantity of input provided (e.g., time spent in the production of services)
ACTIVITY ADJUSTED SUPPLY Ns lij, participation rate of stock, kij, activity rate of participating stock. W FTE hours Stock of providers: Mt-1ij is stock of providers in the previous time period, t-1
PROVIDER REQUIREMENTS Traditional approach: Implicit analytical framework using demography, P, and current level of providers N/P as constant Or, provider-population ratio replaced by service use -population ratio, Q/P .Requires link between services and providers , N ij/Qij, N ij/Qij,, productivity, implicitly assumed constant over time
BEYOND DEMOGRAPHIC CHANGE: AN ENHANCED FRAMEWORK Need for services not part of traditional approach Introducing Hijthe average level of needs in group i , j Determinants of requirements: DEMOGRAPHYPij:Size and age-gender profile of the population EPIDEMIOLOGY Hij/Pij : levels and distribution of needs in the population LEVEL OF SERVICE Qij/Hij : the level of service associated with each level of need PRODUCTIVITY Nij/Qij : the inverse of the average level of productivity of providers serving population group Pij
NEEDS BY AGE ACROSS COHORTS • Data from multiple pop health surveys (1994-2005) • For each year, estimate health indicator by age and sex • Single data set describes health by age and birth year • Regression models used to describe how the age pattern of health varies by birth cohort and sex • Health indicators: • Mortality, morbidity,self-assessed health (55-84) • Risks to health (smoking and alcohol use) (25-54)
AGING AND HEALTH OVER TIME • Rates of increase of mortality and mobility problems by age is greater for older cohorts. • more recent birth cohorts are living longer • chance of having mobility problem at 70 is 6.7% for male born 1939 but 7.8% born in 1921 • Increasing probability of pain with age but lessening over time • Increasing probability of reporting poor health by age but constant over time
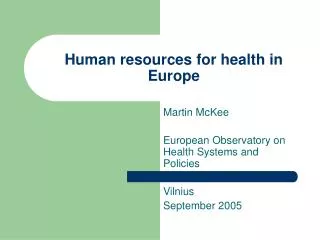
APPLYING THE ANALYTICAL FRAMEWORK: SIMULATION MODELS General simulations: Illustrate relative and combined impacts of different policies Software:Vensim Population: Combined Atlantic provinces Needs: Age-gender levels of health Scenarios: constant, trend, Canada Providers: Hypothetical profession 2 different age distributions (Data taken from several professions) Planning period: 40 years
9000 8000 7000 6000 (1) (2) Total Activity-Adjusted Providers 5000 (3) 4000 (4) 3000 Mature Provider Distribution, Low Exit Rates (1) Mature Provider Distribution, High Exit Rates (2) 2000 Young Provider Distribution, Low Exit Rates (3) 1000 Young Provider Distribution, High Exit Rates (4) 0 0 5 10 15 20 25 30 35 40 Future Years TOTAL ACTIVITY-ADJUSTED PROVIDERS OVER TIME
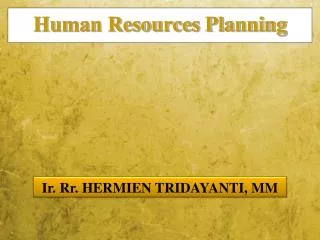
Status Quo (500 Seats) (1) … With Other Improvements* (3) Increase Training Seats By 20% (to 600) (2) Increase Training Seats By 50% (to 750) (4) … With Other Improvements* (5) EFFECT OF TRAINING SEAT SCENARIOS ON PROVIDER GAP
Potential Policy Scenario Remains Constant Observed Trends Canadian Levels Increase training seats only 130 123 101 Decrease grad out-migration By 20% (from 50% to 40%) 97 90 73 Increase in-migration by 10% 93 85 63 Decrease exit rates by 10% 88 79 59 Shift 20% of 'part-time' to 'full-time' -ve -ve -ve Increase productivity by 0.5% per year (compounded) 73 68 48 ADDITIONAL TRAINING SEATS REQUIRED TO ELIMINATE PROVIDER GAP IN 15 YEARS Needs Scenario
Potential Policy Scenario Need Remains Constant Need Follows Observed Trends Need Conforms to Canadian Levels Make no other changes (baseline) 130 Diff 123 Diff 101 Diff Decrease grad out-migration By 20% (from 50% to 40%) 97 33 90 33 73 28 … AND increase in-migration by 10% 65 32 59 31 42 31 … AND decrease exit rates by 10% 29 36 23 36 7 35 … AND shift 20% of 'part-time' to 'full-time‘ -ve -ve -ve … AND increase productivity by 0.5% per year (compounded) -ve -ve -ve ADDITIONAL TRAINING SEATS PER ANNUM REQUIRED TO ELIMINATE PROVIDER GAP IN 15 YEARS UNDER COMBINIATION OF POLICIES
SUMMARY Separates the roles of changes in population demographics, levels of health, levels of service and productivity on the determination of HHR requirements Avoids ‘illusions of necessity’ (or Roemer’s Law) in planning HHR and hence perpetuating imbalances in HHR Provides a basis for considering the impact of health care policies on HHR