Download
1 / 21
210 likes | 315 Views
T he investment framework - Critical enablers are not a luxury!. Bernhard Schwartlander. Good progress towards 15 million people on antiretroviral treatment by 2015. Source: UNAIDS, 2012. Good progress towards elimination of new HIV infections among children (0–14 years) by 2015.

E N D
The investment framework - Critical enablers are not a luxury! Bernhard Schwartlander
Good progress towards 15 million people on antiretroviral treatment by 2015 Source: UNAIDS, 2012
Good progress towards elimination of new HIV infections among children (0–14 years) by 2015 Source: UNAIDS, 2012
Maternal access to ARVs needs to be consistent, to boost coverage during breastfeeding Percentage of eligible mother-child pairs receiving effective prophylaxis to prevent new HIV infections among children, low- and middle-income countries, 2011 29% During pregnancy and delivery During breastfeeding Source: UNAIDS, 2012
HIV incidence: we are NOT on track to achieve the goal of reducing adult HIV infections by half by 2015 Source: UNAIDS, 2012
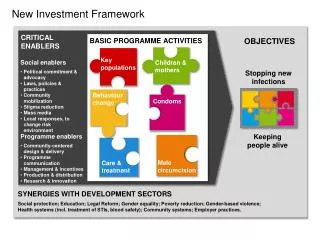
AIDS: investing strategically to maximize impact OBJECTIVES BASIC PROGRAMME ACTIVITIES Child infections & maternalmortality Keypopulations Stopping new infections Behaviour change CRITICAL ENABLERS Condoms • Social • Programme Keeping people alive Male circumcision Treatment & care SYNERGIES WITH DEVELOPMENT SECTORS
Optimized investment could lead to rapid declines in new HIV infections Current and projected number of new HIV infections Vietnam Nigeria Cambodia Baseline Investment approach 2015 2015 1990 2015 1990 1990 South Africa Zimbabwe Ukraine 1990 2015 2015 1990 2015 1990 Source: UNAIDS 2011
Critical enablers and development synergies are distinct, but on a continuum Development synergies HIV-specific (sole or primaryobjective is anHIV-related outcome) HIV-sensitive (HIV outcomeis one of manyobjectives) Critical enablers
Value for money: doing the right things 300 000 Russian Federation Number of new HIV infections Brazil - 1980 1990 2000 2010 Source: UNAIDS
Morocco: reallocation to invest where the epidemic is happening 80 Spending on HIV prevention (2008) Font size!!!!!! People acquiring HIV infection (2009) Percenetage (%) Proposed spending, National Strategic Plan for 2012–2016 0 IDU General population Sex workers and clients MSM Key populations (other) Source: Morocco Ministry of Health, National STI/HIV Programme, HIV modes of transmission in Morocco. August 2010.
Significant reductions in cost for HIV treatment Costs for facility-level ART including costs for ARVs, personnel, labs, training, etc. Cost per person/year US$ Sources: Menzieset al 2011; CHAI, 2012; Bollinger & Adesina, 2011
Community support keeps people on treatment CLINIC-BASED TREATMENT 70% still receiving treatment after two years Sub-Saharan Africa: people receiving ART from specialist clinics Source: Fox MP, Rosen S. Patient retention in antiretroviral therapy programs up to three years on treatment in sub-Saharan Africa, 2007–2009: systematic review. Tropical Medicine and International Health, 2010, 15(Suppl. 1):1–15. COMMUNITY TREATMENT MODEL 98% still receiving treatment after two years Mozambique: self-initiated community model Source: Decroo T et al. Distribution of antiretroviral treatment through self-forming groups of patients in Tete province, Mozambique. Journal of Acquired Immune Deficiency Syndromes, 2010 [Epub ahead of print]. Sources: Fox MP, Rosen S. Tropical Medicine and International Health, 2010. DecrooT et al. Journal of Acquired Immune Deficiency Syndromes, 2010.
Community mobilization increases effectiveness Community mobilisation increased HIV testing rates four-fold in Tanzania, Zimbabwe, South Africa and Thailand Consistent condom use in the past 12 months was 4 times higher in communities with good community engagement (Kenya) Hypothetical circumcision model KwaZulu-Natal : • Core intervention: 240,000 infections averted over ten years • With enablers: 420,000 infections averted, with modest marginal increase in costs
Legal literacy (know your rights and laws) Legal services Law reform Stigma reduction Policetraining on non-discrimination, space for outreach, non-harassment, etc. Health care worker training on non-discrimination, informed consent, confidentiality, duty to treat, infection control Elimination of violence against women and harmful gender norms Critical enablers improve the legal and social environment
Percentage of people retained in treatment and care after diagnosis, USA 100% USA Retained in treatment and care 0 Diagnosedwith HIV Eligiblefor ART InitiatedART Adherentor undetectable Linked/enrolled in care Tested <30 days Retained in care Source: Gardner E M et al. Clin Infect Dis. 2011;52:793-800
Percentage of people retained in treatment and care after diagnosis, USA and Mozambique 100% USA Mozambique Retained in treatment and care 0 Diagnosedwith HIV Eligiblefor ART InitiatedART Adherentor undetectable Linked/enrolled in care Tested <30 days Retained in care Source: Gardner E M et al. Clin Infect Dis. 2011;52:793-800; Micek et al JAIDS 2009
Percentage of people retained in treatment and care after diagnosis, USA and Mozambique • To improve testing: • Reduce stigma in the community and in healthcare settings • Strengthen community support and referral networks • Enhance human rights literacy 100% USA Mozambique Retained in treatment and care 0 Diagnosedwith HIV Eligiblefor ART InitiatedART Adherentor undetectable Linked/enrolled in care Tested <30 days Retained in care Source: Gardner E M et al. Clin Infect Dis. 2011;52:793-800; Micek et al JAIDS 2009
Percentage of people retained in treatment and care after diagnosis, USA and Mozambique • Improve enrolment in care: • Expand community-centred delivery • Overcome cost & transport barriers • Enhance treatment & rights literacy 100% USA Mozambique Retained in treatment and care 0 Diagnosedwith HIV Eligiblefor ART InitiatedART Adherentor undetectable Linked/enrolled in care Tested <30 days Retained in care Source: Gardner E M et al. Clin Infect Dis. 2011;52:793-800; Micek et al JAIDS 2009
Percentage of people retained in treatment and care after diagnosis, USA and Mozambique • Get more people on treatment: • Enhance peer support programmes • Reduce costs • Overcome transport barriers • Ensure adequate nutrition • Reduce stigma in healthcare settings 100% USA Mozambique Retained in treatment and care 0 Diagnosedwith HIV Eligiblefor ART InitiatedART Adherentor undetectable Linked/enrolled in care Tested <30 days Retained in care Source: Gardner E M et al. Clin Infect Dis. 2011;52:793-800; Micek et al JAIDS 2009
Percentage of people retained in treatment and care after diagnosis, USA and Mozambique • Retain people on treatment: • Adherence support programmes • Reduce gender inequalities • Reduce fear of disclosure • Overcome cost and transport barriers • Referral and support programmes for migrants 100% USA Mozambique Retained in treatment and care 0 Diagnosedwith HIV Eligiblefor ART InitiatedART Adherentor undetectable Linked/enrolled in care Tested <30 days Retained in care Source: Gardner E M et al. Clin Infect Dis. 2011;52:793-800; Micek et al JAIDS 2009