Download
1 / 3
30 likes | 165 Views
Patient Receives Care in the ED or 23/59 Observation Unit. DRAFT. SMOOTH COMMUNICATIONS OVERVIEW Cohesive plan of care between transitions at arrival and discharge from the hospital ( Stay of less than 24 hours ). Hospital Care Summary (electronic/faxed SNF and/or PC).

E N D
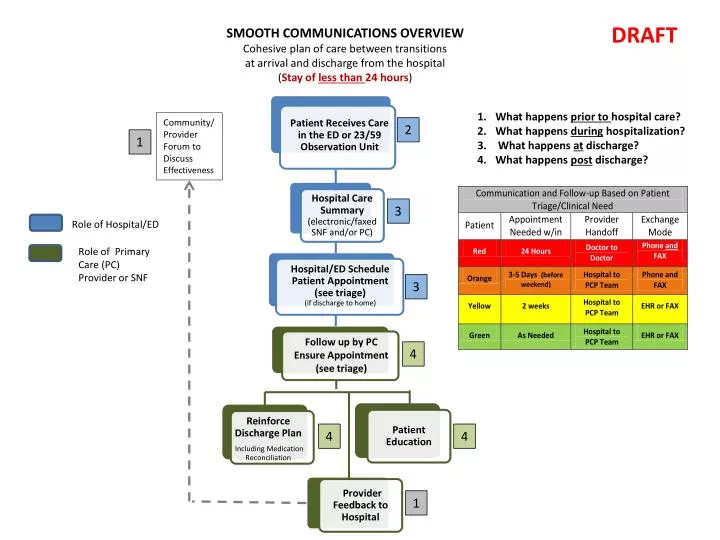
Patient Receives Care in the ED or 23/59 Observation Unit DRAFT SMOOTH COMMUNICATIONS OVERVIEW Cohesive plan of care between transitions at arrival and discharge from the hospital (Stay of less than 24 hours) • Hospital Care Summary (electronic/faxed SNF and/or PC) What happens prior to hospital care? What happens during hospitalization? What happens at discharge? What happens post discharge? Community/ Provider Forum to Discuss Effectiveness 2 1 • Hospital/ED Schedule Patient Appointment(see triage) • (if discharge to home) 3 Role of Hospital/ED • PatientEducation Role of Primary Care (PC) Provider or SNF • Reinforce Discharge Plan • Including Medication Reconciliation 3 • Provider Feedback to Hospital • Follow up by PC • Ensure Appointment(see triage) 4 4 4 1
Patient Receives Care in Hospital DRAFT SMOOTH COMMUNICATIONS OVERVIEW Cohesive plan of care between transitions at arrival and discharge from the hospital (Stays more than 24 hours) What happens prior to hospital care? What happens during hospitalization? What happens at discharge? What happens post discharge? • Patient and Care Giver Communication • PC Notified of • Admission 2 Community/ Provider Forum to Discuss Effectiveness 1 • Discharge Plan (electronic/faxed SNF and/or PC) • Specifics onDischarge Plan including Medications • Education Role of Hospital Role of Primary Care (PC) and SNF 2 2 • Hospital Schedule Patient Appointment(see triage) • (if discharge to home) • Provider Feedback to Hospital • Hospital Follow Up Call to Patient 3 3 3 • Patient and Care Giver Education • Reinforce Discharge Plan • and Medication Reconciliation 4 3 • Follow up by PC • Ensure Appointment(see triage) 4 4 4 1
Smooth Communications – Transitions in Care Discussion Questions • What happens when the patient does not have a primary care provider? • Do we need a separate flow diagram and agreed upon expectations for who does what andwhen in this situation which is fairly common? • How will this change the expectations regarding appointments and the timing of follow-up? • Do we need specific, agreed-upon criteria that will guide the clinical triage of patients at the time of discharge? Or, is it okay to leave this to the clinical judgment of the discharging provider? • What strategies are likely to be most effective in building accountability and responsiveness among community physicians for their proactiveparticipation in the patient hand-off’s? • What are the barriers for community physicians and how can we overcome them most effectively? • What do community physicians need to be most effective? • Are hospitals/emergency departments organized and resourced in the most effective way to effectively facilitate the hand-off’s and provide information? • What do hospitals/emergency departments need to be most effective?