Download
1 / 18
190 likes | 437 Views
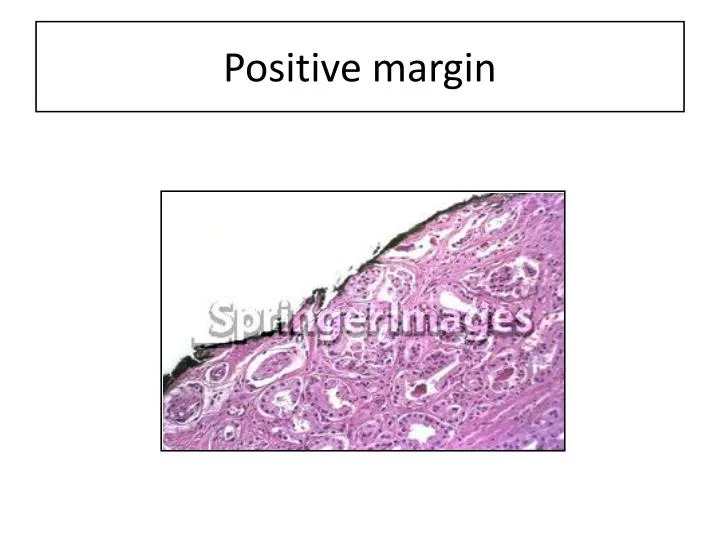
Positive margin. Margin status. If the surgical margin finding is positive should be stated explicitly (although this finding is not relied upon for pathologic staging). specific locations of the positive margins should be reported, and

E N D
Margin status If the surgical margin finding is positive • should be stated explicitly (although this finding is not relied upon for pathologic staging). • specific locations of the positive margins should be reported, and • it should be specified whether EPE or intraprostatic incision is present at each site of margin positivity. • There should be some indication of the extent of margin positivity. NOTE:Positive surgical margins should not be interpreted as extraprostatic extension.
Pathologic Staging (pTNM) (Note K) TNM Descriptors (required only if applicable) (select all that apply) ____ m (multiple) ____ r (recurrent) ____ y (post-treatment) Primary Tumor (pT) ___ Not identified ___ pT2: Organ confined *___ pT2a: Unilateral, involving one-half of 1 side or less *___ pT2b: Unilateral, involving more than one-half of 1 side but not both sides *___ pT2c:Bilateral disease ___ pT2+ ? pT3: Extraprostatic extension ___ pT3a: Extraprostatic extension or microscopic invasion of bladder neck ___ pT3b: Seminal vesicle invasion ___ pT4: Invasion of rectum, levator muscles and/or pelvic wall (Note J) Note: There is no pathologic T1 classification. Subdivision of pT2 disease is problematic and has not proven to be of prognostic significance. Regional Lymph Nodes (pN) ___ pNX: Cannot be assessed ___ pN0: No regional lymph node metastasis ___ pN1: Metastasis in regional lymph node or nodes ___ No nodes submitted or found Number of Lymph Nodes Examined Specify: ____ ___ Number cannot be determined (explain): ______________________ Number of Lymph Nodes Involved Specify: ____ ___ Number cannot be determined (explain): ______________________ Diameter of largest lymph node metastasis: ____ (mm) Distant Metastasis (pM) ___ Not applicable ___ pM1: Distant metastasis ___ pM1a: Nonregional lymph nodes(s) ___ pM1b: Bone(s) ___ pM1c: Other site(s) with or without bone disease Protocol for the Examination of Specimens from Patients with Carcinoma of the Prostate GlandProtocol applies to invasive carcinomas of the prostate gland. Based on AJCC/UICC TNM, 7th editionProtocol web posting date: February 1, 2011
Missing carcinoma???? 1. perform immunostains on any suspicious foci 2. perform levels on blks with HGPIN 3. perform levels x3 on sextant and adjacent sextant regions of prostate where ca identified on biopsy 4. flip the block in these regions and perform three additional levels
Immunoprofile Prostate specific antigen (PSA) - a minority of higher grade prostatic adenocarcinomas are PSA negative, although some of these tumours have been shown to express PSA mRNA. - some prostatic adenocarcinomas lose PSA immunoreactivity following androgen deprivation or radiation therapy
Immunoprofile • Extraprostatic tissues variably immunoreactive for PSA, include • urethral and periurethral glands (male and female), urothelial glandular metaplasia (cystitis cystitica and glandularis), anal glands (male), urachal remnants and neutrophils. • Extraprostatic neoplasms and tumourlike conditions occasionally immunoreactive • for PSA include • urethral/periurethral adenocarcinoma (female), bladder adenocarcinoma, extramammary Paget disease of the penis, salivary gland neoplasms in males (pleomorphic adenoma, • mucoepidermoid carcinoma, adenoid cystic carcinoma, salivary duct carcinoma), • mammary carcinoma, mature teratoma, and some nephrogenic adenomas
Immunoprofile Prostate specific acid phosphatase (PAP) Immunohistochemistry for PAP is active in formalin-fixed, paraffin-embedded tissues. The polyclonal antibody is more sensitive, but less specific than the monoclonal antibody. - PAP and PSA have similar diagnostic utility; - small number of prostatic ca are immunoreactive for only one of the two markers, Extraprostatic tissues reported to be immunoreactive for PAP include: pancreatic islet cells, hepatocytes, gastric parietal cells, some renal tubular Epithelial cells and neutrophils. Neoplasms with immunoreactivity for PAP include: some neuroendocrine tumours (pancreatic islet cell tumours, gastrointestinal carcinoids), mammary carcinoma, urothelial adenocarcinoma, anal cloacogenic carcinoma, salivary gland neoplasms (males) and mature teratoma
Immunoprofile High molecular weight cytokeratins detected by 34βE12 (Cytokeratin-903) is positive in only basal cells Prostatic secretory and basal cells are immunoreactive for antibodies to broad spectrum and low molecular weight cytokeratins.
Immunoprofile 34βE12 is also immunoreactive against squamous, urothelial,bronchial/pneumocyte, thymic, some intestinal and ductal epithelium (breast, pancreas, bile duct, Salivary gland, sweat duct, renal collecting duct), and mesothelium.
Advanced disease • Metastatic prostatic adenocarcinoma can present as bone pain, mainly in the • pelvic bones and spinal cord, where it can cause cord compression but most often asymptomatic. • Enlarged lymph nodes, usually pelvic, but rarely supraclavicular or axillary (typically left sided), • Can sometimes be a presenting symptom. • Ascites and pleural effusion are rare initial presentations of prostate cancer.
Advanced disease • The most common sites of metastatic spread of prostatic carcinoma are - the regional lymph nodes (obturator and hypogastric followed by external iliac, common iliac, presacral, and presciatic nodes ) and - bones of the pelvis and axial skeleton Metastasis to bone marrow, with an osteoblastic response, is a hallmark of disseminated prostate cancer. The bones most frequently effected are: pelvic bones, dorsal and lumbar spine, ribs, cervical spine, femur, skull, sacrum, and humerus. Visceral metastatic deposits in the lung and liver=not often clinically apparent, but common in end-stage disease • Periprostatic/periseminal vesicle lymph nodes may be the first ones to harbour metastatic carcinoma, but in less than 5% of radical prostatectomy specimens.
Partin’s table Partin's table risk groups