Download
1 / 24
280 likes | 791 Views
“Just throw a blanket on him” Causes, Detection, and Treatment of Suspected Transfusion Reactions. Shannon Long, MT(ASCP)SBB Lead Reference Technologist LifeShare Blood Centers. Transfusion Reaction. Definition:

E N D
“Just throw a blanket on him”Causes, Detection, and Treatment of Suspected Transfusion Reactions Shannon Long, MT(ASCP)SBB Lead Reference Technologist LifeShare Blood Centers
Transfusion Reaction Definition: Any unfavorable transfusion-related event occurring in a patient during or after transfusion of blood components
Types of Transfusion Reactions Hemolytic Transfusion Reactions (HTR) Immediate Delayed
Types of Transfusion Reactions (cont’d) Immediate Nonhemolytic Transfusion Rxns Febrile Allergic Anaphylactic and Anaphylactoid Rxns Pulmonary Edema Circulatory Overload Bacterial Contamination
Types of Transfusion Reactions (cont’d) Delayed Nonhemolytic Transfusion Reactions Alloimmunization Post-transfusion Purpura Transfusion-Associated Graft vs. Host Iron Overload Immunosuppression
Pathophysiology 1 – 2 hrs. post transfusion RBCs rapidly destroyed ABO, K, Jka, Fya Intravascular Extravascular Signs & Symptoms Fever, Chills Nausea, Vomiting Chest, Back pain Hemoglobinemia Hemoglobinuria Shock DIC Immediate Hemolytic Transfusion Reaction
Therapy Physician should monitor the patient closely for risk factors to DIC, hypotension, and acute renal failure Mannitol to induce renal diuresis Dopamine for hypotension Blood components for coag abnormalities or DIC Immediate Hemolytic Transfusion Reaction (cont’d)
Immediate Hemolytic Transfusion Reaction (cont’d) Prevention • Because most IHTRs are caused by clerical error, the are potentially preventable. • Therefore, do follow procedures for specimen collection, labeling, and testing, and procedures for issuing blood components. • Follow transfusion policies and procedures.
Pathophysiology 3-5 days post transfusion Anamnestic response Primary alloimmunization Rh, Kell, Fya Extravascular Signs & Symptoms Mild fever and chills Moderate jaundice Slight anemia Hemoglobinuria Rare: Shock and Renal failure Delayed Hemolytic Transfusion Reaction
Febrile Nonhemolytic Transfusion Reaction Definition A 1°C temperature rise associated with transfusion and having no medical explanation other than blood component transfusion.
Febrile Nonhemolytic Transfusion Reactions (cont’d) Pathophysiology • FNHTRs are caused by leukocyte antibodies present in the patient’s serum • Leukocyte antibodies are commonly directed against antigens present on monocytes, granulocytes, or lymphocytes • These antibodies are predominantly HLA or lymphocytotoxic antibodies
Signs & Symptoms Fever and Chills Hypotension (rare) Need to exclude: IHTR Bacteremia Medications Another Illness Prevention Leukocyte-reduced blood products Premedication with acetominophen to patients with documented histories of FNHTR. Febrile Nonhemolytic Transfusion Reactions (cont’d)
Allergic (Urticarial) Transfusion Reactions Pathophysiology • Donor plasma has foreign allergens that react with IgE or IgG in patient plasma, or vice versa. • Histamine is released increasing vascular dilation and permeability. • Swelling, Redness, and Itching develops
Signs & Symptoms Redness Itching Hives Rarely Fever Severe Cases: Angioneurotic edema, laryngeal edema, bronchial asthma Therapy Benadryl Plasma-deficient blood components Allergic (Urticarial) Transfusion Reactions (cont’d)
Anaphylactic and Anaphylactoid Reactions Pathophysiology • Reactions are attributed to IgA deficiency in patients who have developed anti-IgA antibodies by sensitization from transfusion or pregnancy. • Despite the fact that about 1 in 700 people have some level of IgA deficiency, anaphylactic reactions are rare. • Reactions are mediated by histamines and leukotrienes.
Anaphylactic and Anaphylactoid Reactions (cont’d) Signs and Symptoms Anaphylactic • Patients are deficient in IgA, with class specific IgA antibodies • Sudden onset with pronounced symptoms of coughing, dyspnea, nausea, emesis, bronchospasm, flushing of skin, chest pain, hypotension, shock, and possibly death Anaphylactoid • Patients have normal levels of IgA, but have a limited type-specific anti-IgA that reacts with light chain of the donor’s IgA • Less severe with symptoms of urticaria, periorbital swelling, dyspnea, and perilaryngeal edema
Therapy Stop transfusion Keep IV line open with saline Epinephrine Coritcosteroids Maintain airway Prevention Remove all plasma from blood components, or Transfuse IgA deficient blood components Anaphylactic and Anaphylactoid Reactions
Transfusion-Related Acute Lung Injury (TRALI) Pathophysiology • Anti-leukocyte antibodies in donor or patient plasma initiate complement-mediated pulmonary capillary endothelial injury. • Anti-leukocyte antibodies react with leukocytes to trigger the complement system to produce C3a and C5a. • Tissue basophils and platelets release histamine and serotonin, resulting in leukocyte emboli aggregating in the lung capillary bed.
Transfusion-Related Acute Lung Injury (TRALI) cont’d Signs and Symptoms • Chills • Cough • Fever • Cyanosis • Hypotension • Respiratory distress • Respiratory failure (severe cases)
Transfusion-Related Acute Lung Injury (TRALI) cont’d Clinical Work-up • Sera from both the donor and patient should be tested for anti-leukocyte antibodies • Diagnosis of TRALI is one of exclusion, such as heart failure, volume overload, bacterial sepsis, and myocardial infarction
Transfusion-Related Acute Lung Injury (TRALI) cont’d Therapy • With adequate respiratory and hemodynamic supportive treatment, TRALI pulmonary infiltrates usually clear after several days. Prevention • Deferral of donors associated with TRALI cases?????? • Deferral of all female plasma donors??????
Other Adverse Effects of Blood Transfusion • Transfusion-Associated Circulatory Overload • Bacterial Contamination Reactions • Physically or Chemically Induced Transfusion Reactions • Alloimmunization • Post-Transfusion Purpura • Transfusion-Associated Graft-Versus-Host Disease • Iron Overload • Immunosupression
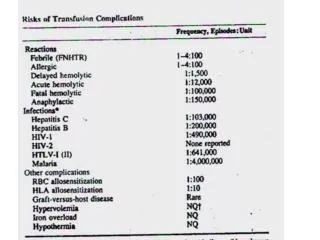
Statistics Rates of Occurrence per unit Transfused NHFTR 1 – 2% Allergic 1 – 2% AHTR 1:25,000 DHTR 1:2,500 Pulmonary edema 1:1000 TA-GVHD 1:39,000 Source: NIH Consensus Conference: Perioperative red cell transfusion. JAMA 260:2700, 1988
Summary • Although adverse effects of blood transfusions are rare, the transfusion service should establish policies and procedures that optimize transfusion practices and provide safety to transfusion recipients with reduced risk of morbidity and mortality. • Regulatory agencies such as CAP and AABB require that written transfusion reaction policies and procedures include steps for detection, evaluation, and reporting of adverse transfusion reactions.