Download
1 / 23
250 likes | 825 Views
Behavioural and Psychological Symptoms of Dementia in Turkey. Engin EKER, MD Istanbul University, Cerrahpaşa Medical School Dept. of Geriatric Psychiatry eneker@istanbul.edu.tr Regional Symposium on Alzheimer’s Disease and Related Disorders in the Middle East October 1-2,2005

E N D
Behavioural and Psychological Symptoms of Dementia in Turkey Engin EKER, MD Istanbul University, Cerrahpaşa Medical School Dept. of Geriatric Psychiatry eneker@istanbul.edu.tr Regional Symposium on Alzheimer’s Disease and Related Disorders in the Middle East October 1-2,2005 Istanbul ,Turkey
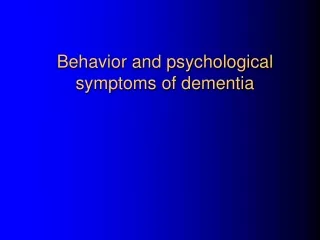
Expected populationof Turkey (million)(OECD projections 1997, SIS 1990 & 2000, DPA 2003)
Elderly Population in Turkey: Highlights Ertan T. IPA Congress.2003 • The proportion of elderly in total population in Turkey is rapidly growing. >60 y: 1990: 7,1% 2003: 10,8% >65 y: 1990: 4,3% 2003: 8% OECD Projection 7,7% in 2020
Behavioral and Psychological Symptoms of Alzheimer Disease • Behavioral -Agression, hostility, agitation: 60% -Apathy: 70% -Wandering and other motor behavior: 30%-40% • Psychological -Depression: 20%-50% -Anxiety: 40%-50% -Hallucinations or delusions: 10%-20% Mega Ms et al. Neurology. 1996;46:130-135; Rubin EH etal. J Geriatr Psychiatry Neurol. 1988;1:16-20; Tariot PN et al. Am J Psychiatry. 1993;150:1063-1069.
Why are BPSD Important • Diminish patient quality of life • Increase caregiver distress: decrease caregiver quality of life( most of the caregivers may have depressive symptoms) • Increase cost of care • Precipitate nursing home placement
Behavioral Precipitants of Nursing-Home Admission Physical aggression 16% Restlessness 13% Verbal outbursts, nonaggressive 13% Verbal outbursts, aggressive 9% Wandering 9% Pacing 3% Other 19% Behaviors that are unlikely to respond to pharmacotherapy: wandering, pacing, screaming, hypersexuality Cohen-Mansfield J 2001; Cohen-Mansfield J. J 1995
The Reasons of Prevalence and Presentation of BPSD in Different Cultures Culturally related factors • The concepts of dementia and behavioural disturbances in society (The typical features of dementia are widely recognized and named “Chinnan (literally childishness) in Kerala (Shaji et al. 2003) • The tolerance of symptoms in dementia • • Not always possible direct observation of the patient by clinician • No cultural appropriateness of rating scales • Availabity of primary and secondary care services for demented patients with BPS • A
Beds for Demented Patients in Turkey • 10% of the beds in all old age homes run by the Health Ministry and Municipalities are spared for demented and physically debilated patients • These patients are separated from the rest of the building • Some voluntary groups are engaged in looking after these patients • The staff working in these parts of old age is well trained
Services for Elderly People With Acute Psychiatric Problems • There are three specialist geropsychiatric unit in Istanbul • The first geropsychiatric unit was organized in Cerrahpaşa Medical School,Istanbul University in 1993 • The elderly with psychiatric problems are mostly placed in general psychiatry departments and are treated by general psychiatrists
Older People and the Informal Health Care System in Turkey • In Turkey, families, friends and neighbours are extensively involved in the care of older people • Demented patients are cared for mostly by their spouses,eldest daughters ,or daughter in-law • Families approach instutional care as a last resort (Eker,1995) • The Directoriate of Social Work and Care has developed a project recently “taking care of the elderly at home”
BPSD in Turkish AD(Eker; Ertan; Engin, 2003) SAMPLE : 213 probable and possible AD cases EVALUATION: DSM-IV (APA, 1994) The Turkish vers. MMSE (Güngen, Ertan, Eker, 1998) GDS (Reisberg et al. 1982) Behave-AD (Reisberg et al. 1987) Neuroimagine technics (CT, MRI) Genetic studies (Apo E4)
Age, Gender, Educational Level, Total BEHAVE-AD Score, the MMSE Turkish Score (in 213 AD Cases) Age, years 74,01±8(45-95) Female, % 68.5 Education, years 7.6 ±5(0-17) Disease duration 4.3 ±3(1-20) The MMSE score 15.6 ±7(0-30) Behave-AD score l0.8 ± 9 (0-47) Patients with symptoms 91.9%
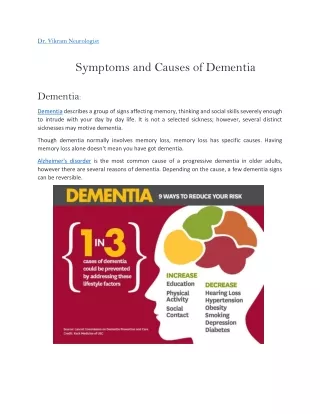
RESULTS (II)Stage Specific Mean BAHAVE-AD in Turkish AD patients Subcategory Scores Stage 3(n:24) Stage 4(n:50) Stage 5(n:74) Stage 6(n:56) Paranoid or delusional ideat 0.75 ±2(0-10) 1.6 ± 1.5(0-7) 1.8 ±1.9(0-7) 4.4 ±3.5(0-15) Hallucinations 0.036 ±0.2(0-1) 0.6 ±1.3(0-5) 0.7 ±1.3(0-5) 1.9 ±2.6(0-13) Activity disturbances 0.42 ±0.9(0-3) 1.6 ±1.8(0-8) 1.7 ±1.8(0-7) 3.7 ±2.8(0-9) Aggressiveness 0.53 ±1.3(0-6) 1.4 ±2(0-7) 1. ±1.7(0-9) 2.5 ±3(0-9) Diurnal rhythm disturbances 0.43 ±0.9(0-3) 0.6 ±1(0-3) 0.4 ±0.9(0-3) 1.3 ±1.4(0-3) Affective Disturbances 0.53 ±0.9(0-3) 1.2 ±1.73(0-5) 0.8 ±1.29(0-6) 1.5 ±1.57(0-6) Anxieties and Phobias 0.75 ±0.9(0-3) 1.8 ±2.26(0-8) 2.08 ±2.1(0-6 2.7 ±2.6(0-11)
Stage specific severity of each Behave AD subcategory in Turkish AD patiens
RESULTS (III)Most Frequent Symptoms in Turkish AD Patients (in 213 cases) % n Purposeless activity 49.3 (105) “People are stealing things” delusion 44.6 (95) Wandering 42.7 (91) Fear of being left alone 40.8 (87) Tearfulness 40.4 (86) Inappropriate activity 38.5 (82) Depressed mood: other 37.6 (80) Anxiety regarding upcoming events 36.6 (78) Verbal outbursts 36.2 (77) Day/night disturbances 33.8 (72) Visual halucinations 26.3 (56)
The 10/66 Dementia Group: Behavioral and Psychologiacal Symptom of Dementia in developing Countries (Int. Psychogeratrics 2004) • Method: Mild and moderate cases (CDR) Main care giver 21 centers in 17 developing countries Community screening Interview for dementia and geriatric mental state schedule (GMS) • Result: At least one BPS was reported in 70,9% of the 555 participants.
The 10/66 Dementia Group: Behavioral and Psychologiacal Symptom of Dementia in developing Countries (Int. Psychogeratrics 2004) • Results: There were regional differences for individual behaviours • High rates of agitation, wandering and sleep distrurbances among Indian participants. • High rates of vocalization among Latin American people with dementia.
The 10/66 Dementia Group: Behavioral and Psychologiacal Symptom of Dementia in developing Countries (Int. Psychogeratrics 2004) • Results: • Overall, numbers of reported BSD were highest in India, intermediate in Latin America and lowest in China. • Depression, anxiety and schizophreniform, paranoid psychosis were commonest among people from Latin America and least common in China.
Delusions in Turkish Patientswith AD:Could Analysing Specific Delusions be MoreHelpful ErtanT, Eker E, Engin F etal.2005(I) • Aim: To analyse factors associated withpresence of delusions to find out whether in individual analysis of delusions in the same group would be more informative • Method :n:185 AD patiens(DSM-IV) MMSE, GDS,Behave-AD Dependent variable :one of the delusions Independent variables: gender,age, education,disease duration,GDS stage ,and presence of each type hallucination,and remaining types of delusions Logistic regression analysis was used
Delusions in Turkish Patients with AD:CouldAnalysing Specific Delusions be Morehelpful(Ertan T,Eker E,Engin F.et al 2005)(II) Result and Conclusions: • None of the delusions was associated with age ,duration of disease ,and education • Female gender was associated with only one delusion (delusions of theft) • Disease stage(GDS :Stage 6) was associated with two delusions(delusion of home is not home and delusion of infidelity( negative association) • Delusions of theft were also independently predicted by delusions imposter and visual hallucination
Conclusions (I) • BPSD is still a novel subject in Turkey. Lack of experienced medical staff in Turkey • Psychiatrists, neurologists, GPs are justhaving necessary information on the subject • AD patients are seen by the psychiatrists and neurologists at late stage (stage 5&6) • Absence of formal services for demented patient • No regular home visit system
Conclusions (II) • Rating scales (Such as GDS;CDR) and measurements for noncognitive symptoms (Behave-AD; NPI; ADAS-non cognitive) are used only by minority neurologists and psychiatrists
Conclusions (III) • There are no trained GP, community nurses, social workers • We should educate family and professional caregivers • We need more validation studies of observer –rated BPSD screening scale • We need cross cultural studies on BPSD developing countries