Download
1 / 31
310 likes | 541 Views
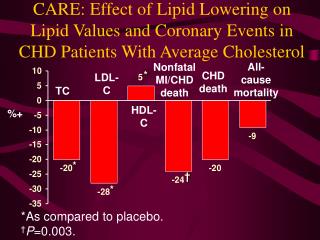
CARE: Effect of Lipid Lowering on Lipid Values and Coronary Events in CHD Patients With Average Cholesterol. All-cause mortality. Nonfatal MI/CHD death. *. CHD death. LDL-C. TC. HDL-C. %+. *. †. *. *As compared to placebo. † P =0.003. CARE: Fatal CHD or Nonfatal MI (Primary End Point).

E N D
CARE: Effect of Lipid Lowering on Lipid Values and Coronary Events in CHD Patients With Average Cholesterol All-cause mortality Nonfatal MI/CHD death * CHD death LDL-C TC HDL-C %+ * † * *As compared to placebo.†P=0.003.
CARE: Fatal CHD or Nonfatal MI(Primary End Point) 15 n=269 Pravastatin Placebo 10 n=206 % with events 5 -24% reduction P=0.002 0 1 2 3 4 5 Yr Sacks FM et al. N Engl J Med. 1996;335:1001-1009.
CARE: Secondary End Points Reductions observed in: % P Confirmed nonfatal MI 23 0.02 MI, fatal and nonfatal 25 0.006 CABG 26 0.005 PTCA 23 0.01 Sacks FM et al. N Engl J Med. 1996;335:1001-1009.
CARE: Impact of Drug Therapy on Lipids and Lipoproteins in Older Patients With MI TC LDL-C TG HDL-C % D P<0.001 for all comparisons with placebo Data from Lewis SJ et al. Ann Intern Med. 1998;129:681-689.
CARE: Reduction in Coronary Events, Revascularizations, and Stroke in Older Adults With MI and Average Cholesterol Levels Major coronary events ‡ Revascular-izations <65 yr (n=2,876) Stroke RR(%) CHD death 65-75 yr (n=1,283) * ‡ † † || ¶ § *P=0.005; †P=0.001; ‡P>0.2; §P=0.004; ||P=0.01; ¶P=0.03. All P values represent within-group differences (treatment vs placebo).
30 30 25 25 20 20 15 15 10 10 5 5 0 0 0 0 1 1 2 2 3 3 4 4 5 5 CARE: Incidence of Coronary Events in Younger Versus Older Patients <65 yr ³65 yr Placebo Placebo %patients Pravastatin Pravastatin -19%P=0.005 -32%P=0.001 Patients at risk, n Placebo 1,435 1,341 1,273 1,194 1,119 265 Pravastatin 1,441 1,357 1,285 1,228 1,177 294 Yr Yr 643 595 559 515 477 119640 590 563 534 505 125
AFCAPS/TexCAPS: Effects of LDL-C Lowering in Patients With Average Cholesterol Levels LDL-C TC UA RV MI C HDL-C % P=0.02 P=0.001 P<0.001 P=0.002
Statin Trials: Therapy Reduces Major Coronary Events in Women 10 Major coronary events* 5 0 -5 -10 -15 % D -20 -25 -30 -35 -34 -46 -46 -40 P=0.012 -45 P=0.001 -50 4S (n=827) CARE (n=576) AFCAPS/TexCAPS (n=997) 2 Prevention 1 Prevention
Overall Risk Reduction for Major Coronary Events by Age: A Meta-analysis No. of Events RRR, % ARR/1000 NNTP PI Statin (95% CI) (95% CI) (95% CI) Value ³65 y740 539 32 (23 to 39) 44 (30 to 58) <0.001 4S 168 122 38 (19 to 53) 98 (43 to 154) 23 <0.001 CARE 111 69 42 (20 to 57) 65 (27 to 103) (17-33) <0.001 LIPID 349 270 25 (11 to 37) 42 (17 to 67) 0.001 AFCAPS 112 78 32 (8 to 49) 21 (5 to 38) 0.01
Overall Risk Reduction for Major Coronary Events by Age: A Meta-analysis (Cont.) No. of Events RRR, % ARR/1000 NNTP PI Statin (95% CI) (95% CI) (95% CI) Value <65 y 1302 951 31 (24 to 36) 32 (24 to 40) <0.001 4S 454 309 38 (27 to 47) 83 (55 to 110) <0.001 CARE 163 143 14 (-9 to 32) 14 (-8 to 37) 31 0.21 LIPID 366 287 25 (12 to 37) 31 (13 to 48) (25-41) <0.001 WOSCOPS 248 174 31 (16 to 44) 23 (11 to 34) <0.001 AFCAPS 71 38 47 (22 to 63) 19 (8 to 31) 0.001
Overall Risk Reduction for Major Coronary Events by Sex: A Meta-analysis No. of Events RRR, % ARR/1000 NNT P PI Statin (95% CI) (95% CI) (95% CI) Value Women 247 180 29 (13 to 42) 33 (13 to 52) <0.001 4S 91 60 37 (10 to 56) 69 (17 to 122) 31 0.01 CARE 39 23 43 (3 to 66) 54 (4 to 104) (19-75) 0.04 LIPID 104 90 15 (-15 to 37) 18 (-16 to 51) 0.30 AFCAPS 13 7 46 (-31 to 78) 12 (-5 to 29) 0.17
Overall Risk Reduction for Major Coronary Events by Sex: A Meta-analysis (Cont) No. of Events RRR, % ARR/1000 NNT P PI Statin (95% CI) (95% CI) (95% CI) Value Men 1795 1310 31 (26 to 35) 37 (29 to 44) <0.001 4S 531 371 38 (28 to 47) 90 (62 to 118) <0.001 CARE 235 189 22 (5 to 36) 26 (5 to 47) 27 0.02 LIPID 611 467 27 (17 to 36) 39 (23 to 55) (23-34) <0.001 WOSCOPS 248 174 31 (16 to 44) 23 (11 to 34) <0.001 AFCAPS <0.001( 710) 109 37 (20 to 50) 22 (10 to 33)
+% stenosis* Event reduction (%) Event Reduction in Angiographic Plaque Regression Trials FATS FATS STARSHARPLCAS (nicotinic acid (lovastatin (diet + resin) (diet + + colestipol) + colestipol) fluvastatin) %
Post-CABG: Impact of Aggressive vs Moderate Lowering of LDL-C on Atherosclerosis Study group characteristics • Sample size: 1,351 (M/F) • 1 to 11 yr post-CABG • 2 patent SVGs (1 in females) • LDL-C 130-174 mg/dL after diet Treatment • Randomized, blinded to • lovastatin 40-80 mg/day + cholestyramine 8 g/day (if needed) • lovastatin 2.5-5 mg/day + cholestyramine 8 g/day (if needed) • aggressive LDL-C target: £85 mg/dL • moderate LDL-C target: 130-140 mg/dL Monitoring • Quantitative coronary angiography
Post-CABG Study:Aggressive vs Moderate Treatment 160 150 Moderate Tx (134-136)* 140 130 LDL-C (mg/dL) 120 110 100 Aggressive Tx (93-96)* 90 80 6 0 12 24 36 48 Follow-up (mo) * Mean achieved. Post-CABG Trial Investigators. N Engl J Med. 1997;336:153-162.
Post-CABG: End Points, Results, Conclusions • Primary end point: Mean per-patient percentage of grafts with significant progression in SVG (³0.6 mm change) • Secondary end point: New occlusions, new lesions, lumen narrowing • Results: • aggressive treatment group: significantly less (P<0.001) progression, fewer new occlusions and lesions, and mean lumen diameter • revascularization rate 29% (P=0.03) • Conclusions: Mean LDL-C levels of 95 mg/dL associated with greater benefit than mean LDL-C of 135 mg/dL Post-CABG Trial Investigators. N Engl J Med. 1997;336:153-162.
Post-CABG Angiographic Outcomes MRE Difference Moderate Aggressive % P value Progression 39 28 28 <0.001 New occlusions 16 10 40 <0.001 New lesions 21 10 52 <0.001 Mean lumen change in mm Minimum diameter -0.38 -0.20 48 <0.001 Mean diameter -0.34 -0.16 52 <0.001 MRE=Mean per-patient percentage of grafts. Post-CABG Trial Investigators. N Engl J Med. 1997;336:153-162.
Post-CABG: Event Rates by Cholesterol Group Event=PTCA or bypass surgery 15 Moderate 10 % Aggressive 5 0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 Yr after enrollment P=0.03.
Effects of Statins on Stroke Events: A Meta-analysis of Primary- and Secondary-Prevention Trials Relative reductionin rates (%) 1° Prevention (-42 to -27)† 2° Prevention (13-45)† Combined (11-40)† *P=0.001.†95% confidence interval of percentage of relative reduction.
Impact of Lowering LDL-C on CVD Events and Total Mortality Nonfatal/fatal CHD CVDmortality % § ‡ † * * *Confidence interval (CI) not reported. †95% CI, 14%-41%. ‡95% CI, 16%-37%. §95% CI, 12%-31%. Hebert PR et al. JAMA. 1997;278:313-321.
Clinical Trial Findings: The Statins • Statins LDL-C by 25%-35% (achieved in clinical event trials and regression studies) • Benefits at various LDL-C levels; evident soon after therapy in some studies • in LDL-C required for in CHD morbidity/mortality • in all-cause mortality in 2° prevention and in cardiovascular mortality in 1° prevention • Studies support treatment in various patient groups • women • elderly • diabetics
VA-HIT Results * % Change * ** * * † *p0.05 **p=0.07 † Investigator designated
A AB B LDL Particle Size Subclass IDL L3 L2 L1 large, buoyant small, dense
Significance of Small, Dense LDL • Low cholesterol content of LDL particles • particle number for given LDL-C level • Associated with levels of TG and LDL-C, and levels of HDL2 • Marker for common genetic trait associated with risk of coronary disease (LDL subclass pattern B) • Possible mechanisms of atherogenicity • greater arterial uptake • uptake by macrophages • oxidation susceptibility
HDL Atherosclerosis Treatment Study (HATS) NIH-funded, the HDL Atherosclerosis Treatment Study is a double-blind, placebo controlled, factorial design, 3-year angiographic trial. Patients (n=160) 15% had diabetes, 10% had impaired glucose tolerance. Patients randomized into four (4) treatment goups: 1. Niacin (2-4 grams/day) + Simvastatin (10-20 mg/day) plus Antioxidant Vitamins 2. Placebo (Niacin+Simvastatin) plus Antioxidant Vitamins 3. Niacin (2-4 grams/day) + Simvastatin (10-20 mg/day) plus Placebo (Vitamins) 4. Placebo (Niacin + Simvastatin) plus Placebo (Vitamins)
HDL Atherosclerosis Treatment Study (HATS) Mean Baseline Lipid Levels: LDL-C 126 mg/dl HDL-C 31 mg/dl Triglycerides 217 mg/dl after Niacin + Simvastatin therapy (average dose: 3.2 gms niacin, 12 mg simvastatin) LDL-C 82 mg/dl reduced 35% HDL-C 40 mg/dl increased 30% Triglycerides 144 mg/dl reduced 34% Niacin+Simvastatin HDL increased 30% LP A-1 increased 75% Niacin+Simvastatin+Vitamins HDL increased 20% LP A-1 increased 17% Antioxidant Vitamins blunted the effect of Niacin+Simvastatin on HDL, specifically HDL2
HDL Atherosclerosis Treatment Study (HATS) Primary quantitative angiographic patient endpoint was the average change in percent stenosis of the 9 worst lesions in 9 standard coronary segments: Placebo + 34% Antioxidant Vitamins + 15% Niacin + Simvastatin + Antioxidants + 7% Niacin + Simvastatin - 4%
HDL Atherosclerosis Treatment Study (HATS) Primary clinical endpoint was the Kaplan-Meier intention-to-treat time to first event: CAD death, MI, Stroke, Hospital-confirmed unstable ischemia + revascularization. 15% of the patients were diabetic while 10% of the patients had impaired glucose tolerance. Patients on Niacin + Simvastatin had clinical events reduced by 70%. The addition of Antioxidant Vitamins to Niacin + Simvastatin resulted in only a 15% reduction in clinical events.
Clinical Benefits of Cholesterol Reduction • A recent meta-analysis of 38 trials demonstrated that for every 10% reduction in TC • CHD mortality decreased by 15% (P<0.001) • total mortality decreased by 11% (P<0.001) • Decreases were similar for all treatment modalities • Cholesterol reduction did not increase non-CHD mortality Gould AL et al. Circulation. 1998;97:946-952.
US Adults Who May Require Drug Therapy for Elevated LDL-C Millions <2 RF andno CHD ³2 RF andno CHD With CHD Total Jacobson TA, et al. Arch Intern Med. 2000;160:1361-1369.