Download
1 / 25
330 likes | 1.3k Views
Endoscopic skull base surgery a brief. Dr.Mohammed Tariq FRCS Associate professor ENt Unit II SIMS Services hospital,Lahore. History. The earliest approaches to brain surgery were at the skull base.

E N D
Endoscopic skull base surgerya brief Dr.Mohammed Tariq FRCS Associate professor ENt Unit II SIMS Services hospital,Lahore.
History • The earliest approaches to brain surgery were at the skull base. • 1870 .. Francesco Durante was the first to remove an olfactory groove meningioma from the skull base in a 35-year-old woman who presented with proptosis, loss of smell, and memory impairment • 1879 ..William Macewen contributed further
Subsequent innovations • Sir Victor Horsley (1857–1916) sectioned the posterior root of the trigeminal nerve for pain relief, • Sir Charles Ballance (1856–1936) reported one of the earliest cases of acoustic tumor removal, • Fedor Krause (1857–1937) from Germany, Thierry de Martel (1875–1940) from France, and others made major contributions to skull base surgery
feasibility With this approach it is possible to expose the intradural cranial base, from the olfactory groove to the odontoid process of C2. The most common surgery related problems are related to the prevention of postoperative CSF leakage and, in cases involving the lower skull base, the usual issues of stability of the craniovertebral junction. Nevertheless, the potential benefits of such an approach, which allows exposure of the surgical area with no skin incision or neurovascular retraction, cannot be overestimated.
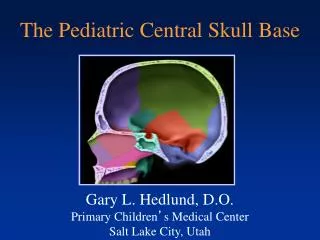
The midline skull base • is an anatomical area that extends from the anterior limit of the cranial fossa down to the anterior border of the foramen magnum. • Resection of lesions involving this area requires a variety of innovative skull base approaches. • These include anterior, anterolateral, and posterolateral routes, performed either alone or in combination, and resection via these routes often requires extensive neurovascular manipulation.
The major potential advantage • it provides a direct anatomical route to the lesion without traversing any major neurovascular structures, obviating brain retraction. • Many tumors grow in a medialtolateral direction, displacing structures laterally as they expand, creating natural corridors for their resection via an anteromedial approach.
Potential disadvantages • the relatively restricted working space • the danger of an inadequate dural repair with cerebrospinal fluid (CSF) leakage .These approaches often require a large opening of the dura mater over the tuberculum sellae and posterior planum sphenoidale, or retroclival space. In addition, they typically involve large intraoperative CSF leaks, which necessitate precise and effective dural closure • potential for meningitis
accuracy and safety • the constant improvements in diagnostic imaging techniques and the increasing use of image guidance systems during endoscopic endonasal procedures has provided increasing accuracy and safety for this approach, allowing improved, constant surgical orientation in an anatomically complex area.
Endoscopic trajectories different areas of the midline skull base exposed through the endoscopic endonasal approach. • to the olfactory groove; • to the sella turcica and planum sphenoidale; • to the clivus • to the craniovertebral junction and foramen magnum.
Currently approach provides • the definitive treatment of choice for most pituitary adenomas, • craniopharyngiomas and meningiomas of the sellar region. • The elegant minimally invasive transnasal endoscopic approach to the sella turcica and the anterior skull base has added a new dimension of versatility to pituitary surgery and can be adapted to many lesions in the region.
removal of pituitary tumors • The refinement of minimally invasive endoscopic techniques has resulted in 'pure' endoscopic endonasal trans-sphenoidal surgery, which is a relatively new approach for the removal of pituitary tumors.
removal of pituitary tumors The technique • wide anterior sphenoidotomy • detachment of the septum from the sphenoid face avoiding the use of a trans-sphenoidal retractor and any intraoral or nasal incisions. • Straight and angled endoscopes are used throughout the procedure to provide a wide view of the sella and are manipulated by a co-surgeon.
an improvement over pituitary microsurgery • decreased post-operative morbidities • a shortened postoperative stay • it eliminates the need for packing • providing an opportunity to monitor the sella after surgery. • It incorporates image-guided surgery, with the fusion of computer tomography and magnetic resonance imaging • employs new and dedicated instrumentation.
Future advancements • in intraoperative imaging, • cranial base reconstruction, and • robotics will make this technique even more successful
unique reconstructive challenges • The creation of large defects of the bone and dura endoscopically presents unique reconstructive challenges. • A layered reconstruction of the dura with inlay and onlay fascial grafts covered with fat grafts is an effective technique for repair. • An intranasal balloon catheter is used to provide counterpressure in the early phase of healing and • a lumbar spinal drain is a useful adjunct in patients at increased risk of a cerebrospinal fluid leak. • Vascularized flaps may be necessary in some patients receiving radiation therapy. • Continued advances in surgical technology and the introduction of new biomaterials will facilitate the reconstruction of skull base defects following surgery.
Endoscopic experience with the repair of small cranial base defects following • trauma, • sinus surgery, and • spontaneous CSF leaks (meningoencephaloceles) has demonstrated a high rate of successful repair using a variety of techniques.
Endoscopic experience 1 Success does not appear to be dependent on the type of reconstructive material, repair technique, or use of lumbar spinal drainage. 2 A special population of patients that appear to be at increased risk of recurrent CSF leak are those presenting with spontaneous CSF leaks. 3 These patients are characteristically obese, middle-aged females and measurement of CSF pressures following repair often confirms occult hydrocephalus. Despite initial success, such patients remain at risk for recurrent CSF leaks months to years following repair
vascularized tissue flaps • Some populations of patients may require reconstruction with vascularized tissue flaps due to the volume of the defect or the lack of vascularized tissue (prior irradiation). • Options include a pedicled pericranial scalp flap, temporoparietal fascial flap, or microvascular free flap
Dural defect following endoscopic craniofacial resection of a neuroendocrine carcinoma of the anterior cranial base.
A synthetic dural substitute (DuraGen) is placed intradurally over the surface of the exposed brain so that the dural edges overlap the inlay graft.
The first fascial graft (Alloderm) is sutured to the dural margins.
Nitinol U-clips are used to anchor the fascial graft to prevent migration or displacement by CSF.
Fat grafts cover the fascia and are in contact with the surrounding bone.
A Foley balloon catheter crosses the nasopharynx posterior to the nasal septum, prior to inflation with saline. The surface of the fat graft is covered with Surgicel to form an adherent crust.