Download
1 / 12
120 likes | 300 Views
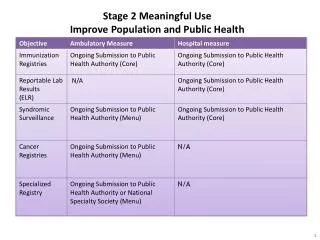
Functional Requirements and Health IT Standards Considerations for STAGE 3 Meaningful Use for Long-Term and Post-Acute Care (LTPAC). Update to the HITPC MU WG – Subgroup #3: Standards & Interoperability: Longitudinal Coordination of Care (LCC) Workgroup (WG) and HL7 Activities. Content.

E N D
Functional Requirements and Health IT Standards Considerations for STAGE 3 Meaningful Use for Long-Term and Post-Acute Care(LTPAC) Update to the HITPC MU WG – Subgroup #3: Standards & Interoperability: Longitudinal Coordination of Care (LCC) Workgroup (WG)and HL7 Activities
Content • Overview: • Standards & Interoperability: Longitudinal Coordination of Care Workgroup (S&I LCC WG) and Sub-workgroup Activities • HL7 Activities • Piloting • S&I LCC Next Steps • Recommendations to the HITPC MU WG – Subgroup #3 (HITPC MU WG – SG #3)
The S&I LCC Initiative -- Overview • The S&I LCC WG: • Collaborates with HL7 and provided input on refinements to Spring 2012 C-CDA ballot to include: functional status, cognitive status, and pressure ulcer content • Collaborates with Keystone Beacon Community and HL7 to identify content and standards needed for Patient Assessment Summary (PAS) Documents and support their on-going and future pilots. • The S&I LCC WG achieved consensus (June 2012) on a “foundational” Use Case that leverages requirements in the Meaningful Use (MU) Program for eligible providers and hospitals to support four clinical document exchanges with LTPAC organizations: • Transfer from Acute Care Hospital to Home Health Care • Referral from Nursing Home to ED • Consult summary for shared care from ED to Nursing Home • Primary care physician and home health care sharing the Home Health Plan of Care (HH POC) • The S&I LCC activities include: • Harmonizing existing standards, including content in the PAS document, and filling gaps, • Developing implementation guides and reference implementations, and • Enlisting pilots with a goal of providing tested IG(s) for the four transactions and documents for MU3 consideration mid 2013. • The S&I LCC WG, in collaboration with HL7, has begun: • preliminary planning for a dynamic “longitudinal” care plan using the HH POC requirements as a foundation; and • an analysis of “care plan” requirements proposed for MU Stage 2.
S&I LCC Workgroup • S&I LCC WG: • Includes 124 total and 63 committed members representing: LTPAC providers and vendors, physicians, nurses, AHIMA, ONC Challenge Grant and Beacon Community recipients, federal representatives (e.g., ASPE, CMS, ONC), and ONC contractor staff • Three sub-work groups: • Patient Assessment Summary (PAS) • Transitions of Care (ToC) • Longitudinal Care Plan (LCP)
Patient Assessment Summary Sub-Workgroup • Focus: Identify standards for interoperable exchange of patient assessment content and patient assessment summary documents to support the care of persons receiving LTPAC services. • Background: • CMS requires that certain providers electronically transmit non-interoperable patient assessment instruments: • Minimum Data Set 3.0 (MDS3.0) for nursing homes (NHs) • Outcome and Assessment Information Set - C (OASIS-C) for home health agencies (HHAs) • In-Patient Rehabilitation Facility- Patient Assessment Instrument (IRF-PAI ) for IRFs. • CMS piloted, in a payment demonstration, the CARE (Continuity Assessment Record & Evaluation) instrument at hospital discharge and at both admission and discharge from post-acute care (PAC)
Status: S&I PAS SWG, HL7 Activities, and Keystone • PAS SWG and HL7 identified refinements to the Consolidate CDA (C-CDA) to represent and transmit: functional status, cognitive status, and pressure ulcers. • The HL7 May 2012 C-CDA ballot now includes templates for the representation and transmission of: functional status, cognitive status, and pressure ulcers. • PAS SWG validated and refined clinically useful subsets of assessment content to support: Transition in Care, Shared Care, and Care Planning. • PAS SWG, Keystone Beacon Community, and HL7 are collaborating to develop a document exchange standard for PAS document. • HL7 will ballot the standard in September 2012 ballot cycle. • Pilot: The Keystone Beacon Community: • Is piloting the exchange of PAS documents using the CCD; and • Beginning in December 2012, will pilot the exchange of PAS documents using the HL7 standard balloted in June and September 2012.
S&I LTPAC Transitions of Care (ToC) Sub-Workgroup and ONC/ MA Challenge Grant • Focus: identify standards needed for the exchange between Eligible Professionals/Eligible Hospitals, LTPAC providers and patients of an interoperable summary document to support transitions in care. • Exchange recipient-defined clinical content for the following identified high-priority transitions: • Acute care hospital to home health • Nursing home to emergency room • Emergency room to nursing home • Leverage and re-use selected data elements from PAS documents, leverage the C-CDA, identify available standards and gaps, and develop an implementation guide and other resources to support the interoperable exchange of an expanded recipient-defined clinical dataset across sites of care. • Status: Work in progress. To be completed December 2012. • Pilot: The ONC MA Challenge Gant (IMPACT): • Beginning in December 2012 will pilot the exchange of this expanded dataset based on the HL7 C-CDA as balloted in June and September 2012.
S&I Longitudinal Care Plan Sub-Workgroup • Focus: Identify standards for the interoperable exchange of care plans focusing on: • Iterative exchange of the Home Health Plan of Care (HH POC) between home care providers and physicians. • Background: The HH POC is nearly ubiquitous among HHAs as it is based on a former CMS POC requirement (i.e., the 485 form). • S&I LCP SWG: Focus on HH POC: structured in collaboration with the Visiting Nurse Services of New York (VNSNY) to support the iterative exchange of the HH POC between: VNSNY, physician practice groups, and other stakeholders. • S&I LCP will leverage the C-CDA, identify available standards and gaps, and develop an implementation guide to support the interoperable exchange of the HH POC between home care providers and physicians. • Identifying components of and standards for a “longitudinal care plan” and relationship of these components to the Meaningful Use EHR program requirements (see slide 10)
Status: S&I LCP SWG: HH POC and VNSNY • Completed: Identified and refined data elements in HH POC. • Activities underway/to be competed: • S&I Harmonization WG will: • Harmonize data elements across S&I ToC documents and PAS documents • Align and harmonize HH POC requirements with “longitudinal care plan” components (see slide 10). • Identify available standards and gaps in standards to support interoperable exchange of HH POC. • Work with HL7 to fill gaps in standards. • Enlist pilots and develop an implementation guide and schema leveraging work under way at the VNSNY to support the interoperable exchange of home care POC. • Status: Work in progress. To be completed December 2012.
S&I LCC WG Next Steps • Recommend that S&I LCC: • Continue its work (described below) to: • identify care plan functional and standards requirements for MU Stage 3; and • identify any gaps in ToC functional requirements and standards for MU Stage 3; and • Provide updates to the HITPC and HITSC on (i) these activities, and (ii) inclusion in C-CDA of templates for: functional and cognitive status, and pressure ulcer, and opportunities to re-use this content/standards for various purposes in MU Stage 3.
Recommendations/Suggestions to theHITPC MU WG – Subgroup #3 The S&I LCC WG recommends that the HITPC MU WG – SG#3 recommend to the HITPC and HITSC that: • The HITPC and HITSC be updated on the inclusion in the HL7 C-CDA of clinical content to support the interoperable exchange of: functional status, cognitive status, and pressure ulcer content. The S&I LCC WG could provide an update on the C-CDA. 2. The HITPC and HITSC consider how MU Stage 3 requirements could/should leverage content and standards for: functional status, cognitive status, and pressure ulcers beyond their use in Care Plans and ToC. 3. The HITPC and HITSC recommend that MU Stage 3 requirements include functional requirements and standards needed on behalf of functionally impaired/ medically complex persons for: • Care plans and needed components, including: defining care plan and identifying and defining needed components (e.g., health concerns, interventions, goals, outcomes, team members, patient preferences, other components); and B. Any needed updates to Summary of Care documents to support transitions of care for these individuals.