Download
1 / 23
230 likes | 466 Views
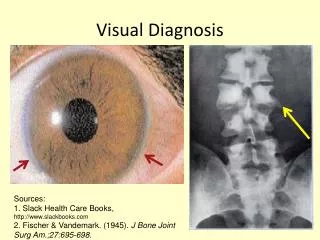
Visual Diagnosis. A Hypoxic Teen Inpatient. Eva Delgado, MD Morning Report. Overview. Case Presentation Work-up based on Differential Significance of the Diagnosis Understanding the Presentation Treating the Pathology Take Home Points. Case Presentation.

E N D
A Hypoxic Teen Inpatient Eva Delgado, MD Morning Report
Overview • Case Presentation • Work-up based on Differential • Significance of the Diagnosis • Understanding the Presentation • Treating the Pathology • Take Home Points
Case Presentation • 16 y/o F with synovial sarcoma in L thigh/hip, metastatic to lungs at diagnosis. • Radiation wound complication, transferred to ortho debridement, revision of hip arthroplasty
Case Presentation • Patient with long course and poor nutrition, so pediatric hospitalist service consulted. • Day peds MD ordered NG tube with local anesthetic and CXR to confirm placement. • RN calls Night peds MD due to desaturation shortly afterward.
Physical Exam • VS: RR 12, O2sat 85-90% on 10L NC • Gen: No ↑WOB, alert • HEENT: No cyanosis • Chest: CTA b/l, good aeration • CV: RRR, no murmur • Ext: wwp, cap refill < 2 sec, • New pulse ox trialed, well-placed, with same reading on different digits
Work-up to Diagnosis • Chart Review: • History- tumor burden/growth, medications, hypercoagulability, similar past episodes • Labs/Studies: • CXR • ABG/VBG • CBC
CBC: Hbg 8.6, HCT 25 VBG: 7.36/44/53/25 -0.1 MetHb: 40% CO-Hb: 0.9% xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Diagnosis: Methemoglobinemia
Hemoglobin = 4 globin chains, 4 heme molecules, each bound to Fe++ A Review of Hemoglobin Oxygen binds Iron (Fe++)
Hemoglobin Methemoglobin • Oxidation = loss of 4 electrons from Fe atoms • Methemoglobin = 4 globin chains, 4 heme molecules, each bound to Fe+++ **Can’t bind O2 in this form**
Significance to Practice • MetHb is 2% of normal blood • Endogenous enzymes reduce to Hb • Methemoglobinemia: • Oxidation >2% MetHb • Oxyhemoglobin curve • Danger: tissue hypoxia *MetHb level 70% fatal
Etiologies of Methemoglobinemia • Congenital: • Deficiency of enzymes that reduce MetHb back to Hb • G6PD Deficiency • Hb M Disease • Diet: • Nitrites from nitrate-rich food or from well water oxidation of Hb
Etiologies of Methemoglobinemia • Meds = most common cause • 42% of 138 cases due to Dapsone • Local Anesthetics: • Prilocaine, Lidocaine, Tetracaine, and… • Topical benzocaine most severe ↑MetHb • Ifosfamide • Bactrim • Methylene Blue* Tobias et al, J of Intensive Care Medicine, 2009.
Presentation: Clinical • No resp distress if MetHb < 20%; +dyspnea > 45% • Cyanosis if MetHb > 15-20% • Hypoxemia manifested as low oxygen saturation on pulse oximetry • SpO2 not responsive to ↑FiO2
Presentation: Serology • Chocolate-colored blood • ABG with normal or high pO2 • AND low O2sat on pulse oximetry • “The Saturation Gap” • VBG with elevated MetHb level Chung et al.J of Emergency Medicine, 2009. Tobias, J of Intensive Care Medicine, 2009.
Pulse Oximetry • Measures O2 saturation of Hb • Sensor contains infrared (940nm) and red (660nm) wavelengths of light • Oxygenated Hb absorbs light at 660nm vs. deoxygenated Hb at 940nm • Ratio of wavelengths absorbed gives O2sat
Pulse Oximetry and Methemoglobin • MetHb absorbs at both wavelengths • MetHb < 20% detected by deoxyHb sensor • MetHb > 20% detected by oxyHb sensor • Newer pulse ox coming with more wavelengths SpO2 = BLUE SaO2 = RED So and Farrington, J Ped Healthcare 2008
Detecting Methemoglobinemia • Co-oximetry: • Measurement of oxygen concentration in blood using numerous UV light wavelengths • Detects oxyHb, deoxyHb, MetHb, carboxyHb
Reducing MetHb • Physiologic response to MetHb: • NADH-dependent MetHb reductase shifts MetHb back to Hb • Rate of conversion = 15%/hour • Infants have small supply of enzyme • Infants and elderly = 50% of Methemoglobinemia cases So and Farrington, J Ped Healthcare 2008
Treating Methemoglobinemia • Poison Control! • Methylene Blue: • Give if symptomatic and MetHb < 20% or if level > 30% • Facilitates reduction via NADPH MetHb Reductase • NADPH enzyme produced by G6PD* • N-acetylcysteine in G6PD Deficiency
Back to the Case • Patient treated with Methylene Blue • Developed chills, rigors, SpO2 70% • No intervention, improved – 96% • Added Benzocaine and Lidocaine to allergy list (along with Ifosfamide) • Risk of recurrence with re-exposure Guay, Anesthesia and Analgesia, 2009.
Low SpO2 and lack of response to ↑FiO2 implies abnormal Hb Don’t forget ABG or VBG, and the saturation gap with normal pO2 Beware local/topical anesthetics Review history and meds if unsure Watch for new pulse oximeters!! Take Home Points
Works Cited • Tobias and Ramachandra, “Intraoperative Diagnosis of Unsuspected Methemoglobinemia Due to Low Pulse Oximetry Values,” Journal of Intensive Care Medicine, July 2009. • So and Farrington, “Topical Benzocaine-induced Methemoglobinemia in the Pediatric Population,” Journal of Pediatric Health Care, 2008. • Chung et al., “Severe Methemoglobinemia Linked to Gel-Type Topical Benzocaine Use: A Case Report,” Journal of Emergency Medicine, 2009. • Guay, “Methemoglobinemia Related to Local Anesthetics: A summary of 242 Episodes,” Anesthesia and Analgesia, 2009. • Bong, Hilliard and Seefelder, “Severe Methemoglobinemia from Topical Benzocaine 7.5% (baby orajel) Use for Teething Pain in a Toddler,” Clinical Pediatrics, 2009. • Mack, “Focus on Diagnosis: Co-oximetry,” Pediatrics in Review, 2007.