Download
1 / 34
340 likes | 455 Views
Endocrine System Disorders, Chapter 21 Converting Between Measurement Systems, Chapter 8: Pages 150 – 152 Calculating Doses of Nonparenteral Medications, Chapter 9: Pages 164-177. Thyroid and Diabetes Ratio-and-Proportion. Mental deviations Changes in energy levels Growth abnormalities

E N D
Endocrine System Disorders, Chapter 21 Converting Between Measurement Systems, Chapter 8: Pages 150 – 152 Calculating Doses of Nonparenteral Medications, Chapter 9: Pages 164-177 Thyroid and Diabetes Ratio-and-Proportion
Mental deviations • Changes in energy levels • Growth abnormalities • Skin, hair, and nail changes • Muscle atrophy (wasting) • Emotional disturbances (mood changes) • Edema • Changes in blood pressure • Sexual irregularities Common Symptoms of Endocrine Diseases
Extremely complex • Involves many organs (regulated by hormones) • seminar will focus on Thyroid disorders and Diabetes Endocrine system
Hypothalamus | \/ TRH Anterior Pituitary | \/ TSH Thyroid Gland** | \/ Thyroid Hormones ------------------ (negative feedback on anterior pituitary) Thyroid Feedback System • TRH- Thyroid Releasing Hormone • TSH- Thyroid Stimulating Hormone • Thyroid Hormones- T3, T4, Calcitonin • **Thyroid gland requires iodine for thyroid hormone formation • Negative feedback: • Increased blood levels-> ant pit releases less TSH • Decreased blood levels-> ant pit releases more TSH
Located in the neck • Made up of 2 ‘lobes’ (on either side of the larynx) • The 3 hormones secreted by Thyroidare … • Thyroxine (T4) • Tri-iodotyhronine (T3) • calcitonin • TSH (Thyroid-Stimulating Hormone) • Secreted by the anterior pituitary gland • TSH controls the secretion of T3 and T4 (see table 21-5 on page 411) Thyroid Gland
Protein synthesis • blood sugar (glucose) levels • serum cholesterol levels • Rate of metabolism • normal mental development and growth • T3 and T4 require iodine for production ! • Diets low in iodine may lead to goiter, enlarged thyroid What do T3 and T4 do?
Causes • Radiation therapy • Lack of iodine • Surgical removal of thyroid • Pituitary dysfunction • Symptoms • Weight gain • Fatigue • Feeling ‘cold’ all the time • Unable to concentrate Hypo (Low) Thyroid levels
Old method: extracted from endocrine glands of animals • New method: Synthetically prepared • Gradually adjust dose for patient needs • Life Long Therapy is the norm … • Can be … (see table 21-2, page 413): • T3 (example Cytomel- liothyronine ) • T4 (example Levothroid/Synthroid/Levoxyl-levothyroxine) • Combo of T3 and T4 (examples thyroid desiccated, Thyrolar) • Approved for supplemental or replacement needs of hypothyroidism Oral Thyroid Replacement
Not used for obesity ! • Doses required for weight loss could be life threatening • Effects of overdose (like hyperthyroidism) • Symptoms include • Psychotic behavior • Diarrhea • Increased blood pressure • Increased heart rates • Cardiovascular reactions • Long term use associated with osteoporosis in post-menopausal women Thyroid Replacement
Life long therapy • Take in the morning on a empty stomach to avoid insomnia. • Palpitations, nervousness, and headaches may be signs of toxicity • Monitor by blood levels • Ok for use in pregnancy Patient Ed: Thyroid Replacements
questions ???? ……….… Questions?
For the treatment of Hyper-thyroid • Hyper-secretion of thyroid hormones • Causes • Tumors • Autoimmune diseases (Graves’ disease) • Symptoms • Increased cell metabolism • Weakness • Anxiety • Heat production Anti-thyroid Medications
Irradiation of thyroid gland • Surgical removal of thyroid • Anti-thyroid Medications: • Interfere with production of thyroid hormones • Iodine or iodide ions • Radioactive iodine (Iodine 131 destroys the thyroid) • Thionamide derivatives • BEWARE!crosses placenta, stops fetal thyroid development! • Removal or destruction of the thyroid will result in the need of life time replacement therapy. • Not as common as Hypothyroidism Cont, Treatment of Hyperthyroidism
… do you have a question? I have a question …
The Pancreas secretes hormones : • Insulin • Glucagon • These hormones regulate metabolism of protein, fat and most importantly carbohydrates • Sixth leading cause of death in U.S. • Effecting >16 million Americans ! Diabetes -Hyperglycemia
Type One Type Two • Juvenile onset • Rapid development • 5-10% of Diabetics • No Insulin produced • Symptoms: Thirst, Urination, and Weight Loss(thin) • Glucose levels fluctuate with activities, illness • Adult onset (>40) • Gradual development • Family History • 90-95 % of Diabetics • Insulin resistance or decreased insulin • May be asymptomatic • Obesity a major factor 2 Types of Diabetes –be able to compare the two types and explain differences !
Diet limiting carbohydrates ( too bad … love those carbs!) • Control body’s use of glucose by consistent exercise, medication. • Drugs fall into 3 categories • Insulin • Oral Hypoglycemic agents • Drugs that affect glucose absorption or production Treatment of Diabetes
Purpose of Insulin • (1)Aids in the utilization of glucose as energy • (2)Prompts the storage of excess glucose as glycogen in liver • (3)Responsible for conversion of glucose to fat. • Decreases blood glucose levels, but if becomes too low, glucagon stimulates the breakdown of glycogen to increase glucose to bring blood sugar levels to normal • Usually given SQ injection • Dose is individualized, and changes over time Insulin
Rapid or Quick Acting • Ex: Insulin Lispro and Insulin Asparte • Onset: 5-minutes, -Duration: ~3hr • Short Acting: Regular Insulin (R) • Onset: 30-minutes, -Duration: ~6hr • Intermediate: NPH Insulin (N) • Onset: 2-hours, -Duration: ~20hr • Long Acting: Lantus Insulin • Onset: 4 to 6-hours, -Duration: ~24hr Insulin Types
Generally well tolerated • May cause allergic reactions • a different product can eliminate this problem • Weight Gain common side effect of Insulin Therapy • Hypoglycemia is the most common side effect • Beware of skipping meals! • Rotate injection sites • Wear medical identification • Patient should ask before taking OTC medications • Monitor blood sugar! Extra-credit: who says … “Check it, check it often … it’s the right thing to do!” Insulin: Patient Education
Have any of these? QUESTIONS
Must have some insulin production in pancreas to use oral medications • Used in Type II after diet and exercise fail • A patient who loses weight may be able to discontinue medication Oral Medications
Sulfonylureas**we will be discussing today • Biguanides • Alpha-glucosidase inhibitors • Thiazolidinediones • Metglitinides • Amulin/GL-1 analogs Classes of Oral Antidiabetic Medications
First oral agents • Two groups • First generation • Second generation • Second Generation • Most potent, effects with lower doses and last longer • Once daily dosing • (See table 21-10 Page 429 for more info) • Examples Glipizide, glyburide Sulfonylureas
No direct insulin activity, increases insulin-secretions (of no use in treatment of Type-I … WHY?) • Most common side effect, Hypoglycemia • More severe with elderly • Must keep strict diet time and well balanced meals • Adverse reactions • Photosensitivity • Jaundice • Rashes • Should not be used in Pregnancy • Become less effective after 10 years use. Many type II’s will have to use insulin for control in later years. • Avoid Alcohol beware disulfram reaction Sulfonylureas continued
Chapters 8 and 9: Converting Between Measurement Systems
…“to change from one form to another” • Necessary in medical field (no world standard) • When numbers are converted from one system to another, they will be approximately equal why Convert ? …
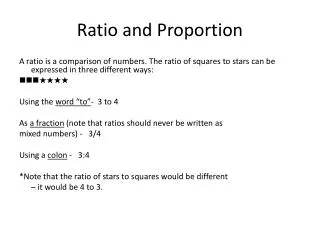
Excellent method! (have I mentioned these are my favorite) ** Please see the ‘practice-sheet’ I made for you in DocSharing. • Ratio—expression comparing two quantities • separated by colon or written as fraction (1:3 or 1/3) • Proportion—comparing two fractions(ratios) considered to be equall • 1:2 and 2:4 same as 1/2 = 2/4 Ratios and Proportions … my favorite!
Numerators must be same units • Denominators must be same units • 1 mL : 15 gtts is the same as 2 mL : 30 gtts • 1 mL/15 gtts = 2 mL/30 gtts Ex: How many gtts in 5 ml’s? 1 ml5ml 15*5=1x 15 gttx gtt 75=1x 75/1 = x x = 75 gtt Solving Unknown Variables
Either method will allow you to solve for X • Notice both are arranged as g/ml (grams/ml) • (both have ‘like’ UNITs in the same position on both sides of the equal sign - Important!) Solving Unknown Variables
A physician orders Tylenol 0.65 gram but when you check your inventory you notice you have Tylenol 325mg tablets. How can you fill this prescription? • 1. How can we make our units equal? • 0.65g => 650mg (move decimal 3 units to the right) • 2.Cross multiply & divide (650mg*1tab / 325mg) to solve for X • X = 2 tab =dose • in other words, 2 of the (325mg tablets) = 650mg =0.65 grams 1 tab X tabx = 2 tab 325mg 650mg cross-multiplying
MD orders penicillin 500mg tid. You check your inventory and have 250mg/5mL solution available.How many teaspoonfuls of medication are needed per dose? Per day? • 1. Ensure units are equal (both are mg’s) • 2. Cross multiply to find out how many ml’s are required per dose (5mL * 500mg / 250mg =10ml’s) 5 mlx mL 250mg 500mg X = 10 ml’s 3. To find out how many teaspoonfuls are needed, convert mL to tsp Remember 5mL=1 tsp, so 10mL = 2tsp 4. 2 tsp’sper dose 5. Since dose is 500mg (2tsp’s) tid need 6 tsp’sper day Volume Conversions
Md writes prescription for metoprolol 12.5mg bid, you have on hand metoprolol 25mg scored tablets. How many tablets would be required for a one month supply (30 days)? • How can you make a 12.5mg dose from 25mg ‘scored’ tablets ? Split them in half each half ( ½ tab) =12.5mg • 12.5mg bid x 30 days ½ tablet bid x 30 days • ½ tab* 2 (twice daily) = 1 whole tablet per day x 30days = 30 whole tabletsfor a one month supply • …hey, what if the directions were to take 12.5mg TID x30 days ? Scored Tablet Practice Problem
2.5 cmx cm 1 in 14 in An abdominal cavity was opened with a 14-inch incision. Convert this measurement into cm (centimeters) • Use this conversion factor: 2.5 cm = 1 inch • 2.5 cm / 1 in = x cm / 14 in • 2.5 x 14 = 35 • 1 x x = 35 • x = 35 • 14 inches = 35 cm Length Conversions