Download
1 / 45
460 likes | 479 Views
Hypertension, or high blood pressure, is a chronic medical condition where blood pressure is abnormally high, requiring the heart to work harder. Learn about primary and secondary hypertension, treatments, medication, and the significance of managing blood pressure levels to prevent complications. Discover risk factors, the increasing prevalence of hypertension, and methods to assess subclinical organ damage.

E N D
„Hypertension” Prof. Dr. János Borvendég CHMP member Hungary
What about Hypertension? • Hypertension or high blood pressure, is a chronic medical condition in which the blood presure in the arteries is higher than it should be. This requires the heartt to work harder than normal to circulat the blood through the blood vessels
Hypertension, also called high blood pressure, condition that arises when the bloodpressure is abnormally high. Hypertension occurs when the body’s smaller blood vessels (the arterioles) narrow, causing the blood to exert excessive pressure against the vessel walls and forcing the heart to work harder to maintain the pressure.
Two types of hypertension. • There are two types of hypertension, called “primary” and “secondary.” Primary hypertension means that the hypertension is not caused by any other disease. Secondary hypertension means that the hypertension is caused by another disease. In most cases (90-95%), hypertension is primary. Only a small amount of hypertension (5-10%) is secondary
The outcome of the hypertension • Although the heart and blood vessels can tolerate increased blood pressure for months and even years, eventually the heart may enlarge (a condition called hypertrophy) and be weakened to the point of failure. Injury to blood vessels in the kidneys, brain, and eyes also may occur.
Bloodpressure is actually a measure of twopressures, thesystolic and thediastolic. The systolicpressure(thehigherpressure and thefirstnumberrecorded) is theforcethatbloodexertsonthearterywallsastheheartcontractstopumpthebloodtotheperipheralorgans and tissues.
The diastolicpressure(thelowerpressure and thesecondnumberrecorded) is residualpressureexertedonthearteriesastheheartrelaxesbetweenbeats. A diagnosis of hypertensionis made whenbloodpressurereachesorexceeds 140/90 mmHg (readas “140 over 90 millimetres of mercury”).
Treatament of hypertension. • Hypertensioncanoften be fixed withchangesindietorlifestyle. • LoseweightiftheyareoverweightorobeseExerciseregularly • Decreasetheamount of salttheyeat • Limit theamount of alcoholtheydrink • Eat a lot of fruit and vegetables.
Medicines • Examples of medications that decrease blood pressure include: • diuretics to get rid of extra fluid • beta receptor and • alfa receptor blocking agents • Ca chanel blockers and • ACE/ inhibitors • AT2 receptor lockers ,
Effectiveness[ • Even small decreases in blood pressure can have a large effect on a person's health. • For example, decreasing blood pressure by 5 mmHg (for example, from 150/100 to 145/95 mmHg) can decrease the risk of stroke by 34%. It can also decrease the risk of heart disease by 21%.[3]
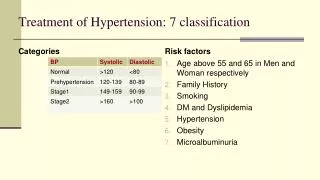
Definitions and Classification of Blood Pressure levels (mmHg) Category Systolic Diastolic Optimal 120 80 Normal 120-129 80-84 High normal 130-139 85-89 Grade 1 Hypertension 140-159 90-99 -”- 2 -”- 160-179 100-109 -”- 3 -”- 180 110 Isolated Systolic Hypertension 140 90
The significance of hypertension • The number of patients with hypertension is growing(!)1988-1991 43,2 mill/US1999-2000 60,0 mill/US - the population ages - obesity - diabetes • Hypertension is the most common risk factor for heart attack and stroke
The significance of hypertension: (cont.) • Only ≈ 34 % of patients with hypertension have their blood pressure controlled.- the HBP remains asymptomatic for long period of time- lack of adherence with the therapy- side effects of the antihypertensive- poor access to medications
Factors influencing the prognosis Risk Factors: S/D BP levels 180/ 110 mmHg Diabetes mellitus Age (M 55 y. F 66 y) Dyslipidemia Abdominal obesity Metabolic syndrome Smoking Snoring / sleep apnoea
Obesity: • Body weight • Increased waist circumference M : 102 cm W: 88 cm • Increased body mass index body weight (kg) / height2(m) overweight 25 kg/m2 obesity 30 kg/m2
Complications: • heart failure • Left ventricular hypertrophy • MI ( myocardialinfarct.) • sudden cardiac death • stroke • intracerebral haemorrhage • chronic renal insufficiency hypertensive nephrosclerosis • retinopathy
Searching for subclinical organ damage • Blood vessels: ultrasound scanning of external carotid arteries ( arteriosclerosis, thickness of intima media), large artery stiffening( pulse wave velocity.
Searching for subclinical organ demage • Heart: ECG (, ischemic condition,arrhythmias, left ventricular hypertrophy), echocardiography ( geometric pattern of remodelling) doppler measurement( diastolic dysfunction). • Kidney: micro/macro albuminuria, se creatinin level, creatinin clearence,glomerular filtration rate, • Brain: MRI/CT ( brain infarct, micro bleeds), cognitive test • Retina :fundoscopy(haemorrhages, exudates,papillo edema)
Laboratory Investigations: fasting plasma glucose/tolerance test se total cholesterol se LDL se HDL fasting se triglycerides se uric acid se creatinine creatinin clearance Hgb/Htc urine analysis (quantitative microalbiminuria) se electrolytes
Determinants of arterial pressure Stroke volumen Cardiac output Heart rate Arterial pressure Vascular structure Perip. resistance Vascular function
Essential (primary hypertension) Pathogenesis: • increased sympathetic neural activity, with enhanced beta-adrenergic activity • increased Angiotensin II. activity and mineral corticoid excess • genetic factors (≈ 30 %) • reduced nephron mass (genetic factors? intra uterine developmental disturbances)
Search for secondary hypertension Measurement of: renin aldosterone, corticosteroids catecholamines arteriographies renal / adrenal ultra sound CT MRI
Goals of Treatment: • Primary goal: to achieve maximum reduction in the long-term total risk of cardiovascular disease • BP should be reduced: 140/90 mmHg (in all hypertensive patients) 130/80 mmHg (in diabetics and in high risk patients) • Antihypertensive th. shouldbe initiated before significant CV damage develops
Choise of antihypertensive drugs • Factors which should be taken into consideration: previous experience of the patients, cardiovascular risk profile of the individual patient, presence of subclinical organ demage(CV,renal, diabetes), presence of co-egsisting disorders, which may limit or contraindicate of using of a particular drug, interaction with the drug considered to be used, cost
Mechanism of Action of AntihypertensiveAgents Diuretics: (?) • Na+ excretion • Plasma volume • Smooth muscle Na+ conc. Outcome: perif. resist. -blockers: • 1/2blocking • 1blocking • MSA (Membrane Stabilisig Activity) • ISA (IntrinsicSympatheticActivity) Outcome: heart ratecardiac outputplasma RAresetting of baro receptors
Mechanism of Action of Antihypertensive Agents (cont.) Alfa antagonists • Selective post synapticic1 blockade Outcome: peripherialresist. preload Ca channel antagonists: • Blockade of voltage sensitive Ca channels • Outcome: peripherial. resist (relax the arterial smooth muscle)
Antihypertensive agents • Diuretics: • thiasides (HCTZ) loopdiuretics( furosemide) aldosteron antagonists ( spironolacton) K+ retaining (amilorid)
Diuretics ( mechanism of action) • Tiazidses inhibit NaCl reabsorption from the luminal side of epithel cells inthe distal, descending convoluted tubules • Loop diuretics selectively inhibit NaCl reabsorption in thick ascending limb of the loop of Henle. This segment has a large NaCl absorptive capacity. They are the most efficacious diuretic agents available
Diuretics ( mechanism of action) • Spironolacton Competitive aldosteronantagonist,antagonizes the effect of aldosteron in the cortical collecting tube and late distal tube.
Antihypertensive agents • Beta blockers non selectives : ( propranolol) selectives: ( metoprolol,bisoprolol) combined alpha/beta blocking agents ( labetolol, carvedilol)
Antihypertensive agents • Alpha 1 antagonists: (prasosin,doxasosin) • Ca++ antagonists: --dihydropyridin deriv.: (nifedipine,amlodipin), --nondihydropiridin.deriv. (verapamil,diltiazem)
Ca channel antagonists (mechanism of action) • Inhibit the Calcium influx into the smooth muscle cells. • Nifedipine(AdalatR)dimethyl-nitrophenyl-dihydropyridineand analogues are more selective as vasodilatators and have less cardiodepressive effects than Verapamil or Diltiazem
RAS (Renin-Angiotensin-System) Kidneys beta blocking agents renin aliskiren Angiotensinogen Angiotensin I ACEiACE Angiotensin II ARB AR aldosteron secretionsympatehic activity Vasoconstriction BP
ACE inhibitors • enalapril(Renitec R )methoxykarbonil-fenilpropil-aminopropanoil-pirolidineperindopril(Coverex R)ethoxicarbonylbutylaminopropanoyl-octahydroindol-carbolicacid
The ACEi-s • inhibition: ( Cardiaceffect)- the LVH (Left Ventricular Hypertrophy)- the myocardial ischemia- glomerular hypertrophy ( Effectonthekidneys)- production of procollagen • mitigate/decrease:( vasculareffet)- deposition of mesangial macromolecules- impairment tubule-interstitial tissues- the endothelial impairment • improve:- the cardiac function- the rheological properties of the blood - the lipid profile- endothelial function- insulin sensitivity
Angiotensine Receptor Blockers • valsartan Diovan R methyl-tetrazol-biphenyl-methylpentaamido-butanoic acid • telmisartanMicardis R bibenzo]imidazol]-methyl-biphenyl]-carboxylic acid • losartan Cozar R ; butyl--chloro-triaza-azanidocyclopenta--dien-phenyl] methyl]imidazol-methanol
Pharmacological effects of ARB-s Blockade of AT1 receptors: Outcome: • vasodilatation- TPR (total Peripheral Resistance) • aldosteron secretion: - Na reabsorption- H2O reabsorption- plasma volume - cardiac output • intra glomerular pressure • release of NA from the synapses - sympathetic tone, neurotransmission • endothelin production • production of A II and renin secretion • stimulation of AT2 receptors (indirectly)
Pharmacological effects of ARBs(cont.) Blockade of AT1 receptors: Outcome: • decrease/mitigate:- LVH (LeftVentricularHypertrophy)- albuminuria (microalbuminuria!)- progression of renalimpairment • protect (?)- CHF- diabeticnephropathy- stroke
Direct renin antagonist mechanism of action: • Aliskiren ( TecturnaR, Rasilez R) Aliskiren by inhibiting directly the ensimatic activity of renin ( produced by the kidneys) blocks the production of Angiotensin.
Pharmacological effects of RI-s Direct blockade of renin enzyme activity • PRA (Plasma Renin Activity) (tissue renin activity ?) • Plasma AT1/AT2 • Aldosterone secretion • BP • - PRC (plasma cc. of renin)
???Effects of RI-s on target organ damage Cardiac:- preventive (cardio protective ??): LVH- curative: CHF Vascular: - protective: endothelial dysfunction against atherogenesis, stroke (??)- improve the elasticity of the large arteries Renal: ( supposed, butnotjustified, )- nephroprotective (in diabetic nephropathy) Metabolic: ( supposed ,butnotjustified)- improve: insulin sensitivitydyslipidemy
Monotherapy versus Combination • Use of more than one agent is necessary to achieve target BP in the majority of patients • Initial treatment can be monotherapyor combination of two drugs (at low doses) with a subsequent increase in doses • Combination of two drugs should be preferred as first step treatment in patients with grade 2/3 range or with high CV risk • In patient with severe hypertension combination of three or more drugs is required
Monotherapy versus Combination strategies Mild/moderateMarked BP elevation BP elevation CV highrisk Singleagent (lowdose)Two-drugcombination (lowdose) previousswitchtodiff. Previous add a third agent (fulldose) agent (lowdose) comb.(fulldose) drug (lowdose) two/three drugcombination mono th. (fulldose) (fulldose) two /threedrug combination (fulldose)