Download
1 / 26
260 likes | 316 Views
Learn about respiratory volumes like Tidal Volume, Inspiratory Reserve Volume, Expiratory Reserve Volume, and Residual Volume, along with respiratory capacities like Inspiratory Capacity, Functional Residual Capacity, Vital Capacity, and Total Lung Capacity. Explore how tests like Spirometry help assess respiratory health and understand nonrespiratory air movements. Discover the transport of oxygen in the blood, the impact of carbon monoxide on hemoglobin, and the role of Red Blood Cells in breathing regulation.

E N D
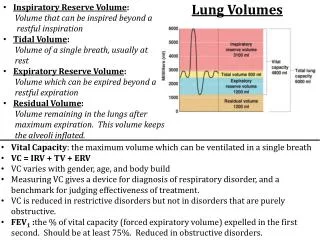
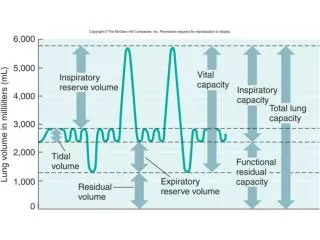
Respiratory Volumes Used to assess a person’s respiratory status • Tidal volume (TV) = The amount of air inhaled or exhaled with each breath under resting conditions • Inspiratory reserve volume (IRV) = The amount of air that can be forcefully inhaled after a normal (TV) inhalation • Expiratory reserve volume (ERV) = The amount of air that can be forcefully exhaled after a normal (TV) exhalation • Residual volume (RV) = The amount of air remaining in the lungs after a forced exhalation
Adult female average value Adult male average value Measurement Description Amount of air inhaled or exhaled with each breath under resting conditions Tidal volume (TV) 500 ml 500 ml Amount of air that can be forcefully inhaled after a nor- mal tidal volume inhalation Inspiratory reserve volume (IRV) 3100 ml 1900 ml Respiratory volumes Amount of air that can be forcefully exhaled after a nor- mal tidal volume exhalation Expiratory reserve volume (ERV) 1200 ml 700 ml Amount of air remaining in the lungs after a forced exhalation Residual volume (RV) 1200 ml 1100 ml Figure 22.16b
Respiratory Capacities • Inspiratory capacity (IC) = Maximum amount of air that can be inspired after a normal expiration: IC= TV+IRV • Functional residual capacity (FRC) = Volume of air remaining in the lungs after a normal tidal volume expiration: FRC = ERV+RV • Vital capacity (VC) = Maximum amount of air that can be expired after a maximum inspiratory effort: VC = TV+IRV+ERV • Total lung capacity (TLC) = The maximum amount of air contained in lungs after a maximum inspiratory effort: TLC = TV+IRV+ERV+RV
Maximum amount of air contained in lungs after a maximum inspiratory effort: TLC = TV + IRV + ERV + RV Total lung capacity (TLC) 6000 ml 4200 ml Maximum amount of air that can be expired after a maxi- mum inspiratory effort: VC = TV + IRV + ERV Vital capacity (VC) 4800 ml 3100 ml Respiratory capacities Maximum amount of air that can be inspired after a normal expiration: IC = TV + IRV Inspiratory capacity (IC) 3600 ml 2400 ml Volume of air remaining in the lungs after a normal tidal volume expiration: FRC = ERV + RV Functional residual capacity (FRC) 2400 ml 1800 ml (b) Summary of respiratory volumes and capacities for males and females Figure 22.16b
Dead Space • Some inspired air never contributes to gas exchange • Anatomical dead space: volume of the conducting zone conduits (~150 ml) • Alveolar dead space: alveoli that cease to act in gas exchange due to collapse or obstruction • Total dead space: sum of above nonuseful volumes
Pulmonary Function Tests • Spirometer: instrument used to measure respiratory volumes and capacities • Spirometry can distinguish between • Obstructive pulmonary disease—increased airway resistance (e.g., bronchitis) • Restrictive disorders—reduction in total lung capacity due to structural or functional lung changes (e.g., fibrosis or TB)
Pulmonary Function Tests • Minute ventilation: total amount of gas flow into or out of the respiratory tract in one minute • Forced vital capacity (FVC): gas forcibly expelled after taking a deep breath • Forced expiratory volume (FEV): the amount of gas expelled during specific time intervals of the FVC
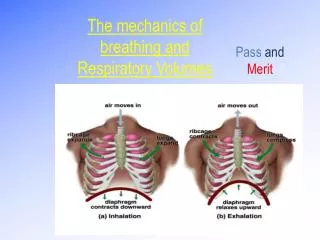
Nonrespiratory Air Movements • Most result from reflex action • Examples include: cough, sneeze, crying, laughing, hiccups, and yawns
Transport of O2 • In each 100ml of oxygenated blood • 1.5% of the O2 is dissolved in the plasma • 98.5% is carried with hemoglobin inside RBC’s as oxyhemoglobin. • 4 molecules of O2 can bind to each hemoglobin
Breathing CARBON MONOXIDE– can occur because CO binds more tenaciously to hemoglobin than O2 does, radically decreasing the oxygen-carrying capacity of the blood and often leading to hypoxia. Carbon Monoxidebinds tightly with Hemoglobin Hemoglobin carriesOxygen and Carbon Dioxide Red Blood Cell
Regulation of Breathing • The rate of Oxygen consumption depends on the activity of the cells. • The rate of Breathing is controlled by the brain which monitors the concentration of Carbonic Acid (HCO3) in the blood. • In other words, CO2 H+ are the controlling factors in rate and depth of respiration…NOT Oxygen!!!
PROBLEMS OF THE RESPIRATORY SYSTEM They may affect the upper respiratory system or the lower bronchial tubes and lungs.
Upper respiratory tract: nose, mouth, sinuses, and throat. Lower respiratory tract: trachea, bronchial tubes, and the structures inside the lungs.
Viral infections • Most common cause of URS(upper respiratory symptoms • Colds and influenza (flu) • Colds: minor URS, usually go away without treatment • Influenza usually more serious than colds; key symptom in adults is fever • Antibiotics are not used to treat viral illnesses
Bacterial Infections • Affect the upper or lower respiratory system • Symptoms tend to localize to one area • Common sites of bacterial infections: Sinuses, Throat, Bronchial Tubes and Lungs • More common in smokers • Treated with Antibiotics
Allergies/Asthma • Symptoms of allergies often last longer than a typical viral respiratory infection • Asthma is a chronic disease of the respiratory system
Pneumonia Causes: Viruses, bacteria, fungi, and parasites. Pneumonia can range in seriousness from mild to life-threatening Antibiotics can treat most common forms of bacterial pneumonias Antibiotic-resistant strains are a growing problem
Chronic Obstructive Pulmonary Disease (COPD) • Includes chronic bronchitis and emphysema • Characterized by irreversible airflow obstruction and often exist together • COPD occurs most often in older people • 80 and 90 percent of COPD is attributed to cigarette smoking
Bronchitis Inflammation of the lining of the bronchial tubes EMPHYSEMA Walls of the Alveoli are damaged Both emphysema and chronic bronchitis cause permanent damage to the lungs and airways
Obstructive Sleep Apnea Causes serious disturbances in normal sleep patterns, patients experience excessive daytime sleepiness and impaired performance Persons affected by OSA, are seven times more likely to be involved in multiple vehicular crashes
CYSTIC FIBROSIS Inherited chronic disease that affects the lungs and digestive system A defective gene and its protein product cause the body to produce unusually thick, sticky mucus that: • Clogs the lungs and leads to life-threatening lung infections; and • Obstructs the pancreas and stops natural enzymes from helping the body break down and absorb food.
Home Treatments for Minor Respiratory Problems • Prevent dehydration • Get extra sleep • Let yourself cough if you have a cough • For a sore throat, gargle at least once each hour
Symptoms to Watch For During Home Treatment • Increasing difficulty breathing • Wheezing develops • New pain develops or pain localizes to one area, such as a sinus area, ear, throat, or chest • Symptoms persist in spite of home treatment • Symptoms become more severe or frequent
PREVENTIONThere is no sure way to prevent respiratory illnesses • Wash hands often • Keep hands away from face • Do not smoke • Exercise regularly • Get a flu shot • Pay attention to pollution indexes avoid asthma triggers To help reduce your risk: