Download
1 / 56
560 likes | 575 Views
The MCB100 Final Exam will take place on Monday, 5/6/19 from 8:00 AM to 11:00 AM. It will cover chapters 26, 11-14, and a small portion of chapter 15. Practice exam available on the course website.

E N D
MCB100 Final Exam Monday, 5/6/19 8:00 – 11:00 AM Last name A - N: Room 112 Gregory Hall Last name O – Z: Room 149 NSRC Conflict Exam IF you have a legitimate excuse, contact Dr. Chapman to sign up. Friday, 5/3 at 8:00 – 11:00 AM Monday 5/6 at 1:30 – 4:30 PM or 7 - 10 PM Tuesday, 5/7 at 8:00 – 11:00 AM in Room 242 Burrill Hall
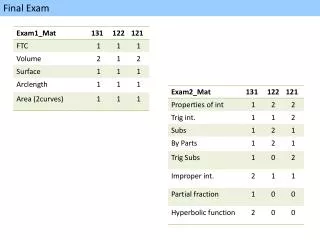
MCB100 Final Exam 50 questions. Multiple choice and matching Machine Graded, 2 points per question See the practice exam at the course web site: From the main index page, click on:“Exam Information” Scroll down to see the link to the practice exam. The exam covers chapters 26, 11 – 14 and a tiny bit of 15. Chapter 26 Applied Microbiology (2 questions) Chapter 11 Prokaryotic Microorganisms (23 questions) Chapter 12 Eukaryotic Microorganisms (10 questions) Chapter 13 Viruses (6 questions) Chapter 14 Infections & Disease (5 questions) Chapter 15 Resistance to Infections (4 questions)
Reading Day – Thursday 5/2/19 Dr. Chapman will be in the Illini Union Courtyard Café From 10:00 AM - Noon (Unofficial Office Hours)
MCB100 Grading Scale Exams300 points are possible Exam 1 100 points Exam 2 100 points Final 100 points LON-CAPA Homework100 points are possible (10 question sets at 10 points per set) (XI is a make-up set, of the 11 sets I drop the lowest score) Group Discussion Participation50 points are possible Add up your points, including your extra credit points. A+ to A- = 450 – 405 points or 100% to 90.0% B+ to B- = 404 – 360 points or 89.9% to 80.0% C+ to C- = 359 – 315 points or 79.9% to 70.0% D+ to D- = 314 – 270 points or 69.9% to 60.0%
MCB100 - INTRODUCTORY MICROBIOLOGY Spring 2019 Chapter 14 Infection, Infectious Disease & Epidemiology
Infection vs. DiseaseDisease = dis + ease (anything that makes you feel bad) An infection is when an undesirable microorganism colonizes the host’s body. Infections can be caused by a wide range of microbes but infections do not always cause disease and some diseases are not caused by infections. Noninfectious DiseasesPneumoconiosis (Black Lung Disease), Intoxication, Coronary Arterial Disease, Severe Combined Immunodeficiency, Strokes, Depression, Alcoholism Infectious Diseases Communicable: Malaria, Flu, Gonorrhea, TB Noncommunicable: Tetanus, Rabies, Lyme Disease
Disease: Signs and Symptoms Symptomsaspects of a disease that are felt by the patientchills, nausea, fatigue, aches & pains Signs indications of disease that can be seen and measured by a physician elevated temperature, vomiting, reduced flexibility or motion, rash spots, inflammation, pus An infection may be asymptomatic, that is without symptoms. picture from cartoonexpress.com
Stages of an Infectious DiseaseEncounterThe microorganism gets into the host. Incubation Period The pathogen begins growing in thehost’s body, no symptoms are seen. Prodromal PeriodFirst symptoms appear, often mild. Illness (aka: Acute Phase)Worst signs and symptoms are seen. Decline (aka: Resolution)Immune response and treatmentreduce the number of pathogens. ConvalescencePatient recovers, this may take time.
Portals of EntryBreaks in the Skin - physical wounds (dirt) (tetanus, gangrene, burn infections) - animal bites (rabies, malaria, Lyme disease, typhus)Mucous membranes - mouth - nose (Strep throat, common cold, TB, flu) - eyes (conjunctivitis, colds, flu) - urogenital tract (bladder infections, STDs) - gastrointestinal tract (diarrheal diseases, ulcers, peritonitis) Trans-placental STARCH
Symbiotic RelationshipsMutualismBoth microbe and host benefit from association. Rhizobium + legume plantsome strains of E.coli + humans CommensalismThe microbe gains a benefit and the host is not harmed or helped. Streptococcus salivarius + humans ParasitismThe microbe gets lunch at the host’s expense. Many disease causing microbes
Opportunistic vs. True Pathogens (aka: frank pathogens) A true pathogen is an infectious microorganism that can cause disease in a healthy human host with a good immune system. An opportunistic pathogen is a weaker infectious agent that can cause disease in a host with weakened resistance/immunity but not generally in a healthy host. What makes an infectious microorganism a true pathogen is the production of virulence factors. Examples of Diseases Caused by True Pathogens: - Diphtheria (Gram + bacteria: Corynebacterium diphtheriae) - Bubonic Plague (Gram – bacteria: Yersinia pestis) - Malaria (protozoan: Plasmodium falciparum) - Yellow Fever (virus –yellow fever virus) Example of a Disease Caused by an Opportunistic Pathogen - hospital acquired septicemia due to Serratia marcescens contamination of IV-TPN solution (Nisbet, Robert (3/30/11) "Drip Feeds Linked To US Hospital Deaths")
Virulence and Virulence Factors Virulence is defined as the ability of a microorganism to cause disease. A virulence factor is a substance that a microorganism produces that increases its ability to infect a host or to cause damage to the host. Most virulence factors are proteins but there are some exceptions to this. Virulence factors fall into two broad categories. Invasins help microorganisms enter a host or evade the host's defenses. Toxins are poisons or enzymes that damage the host.
Examples of Bacterial Virulence Factors and How They Increase Disease - flagella: Flagella allow bacteria to be move. Motility helps the bacteria to spread and this is important in some infections. For example: Esherichia coli and Proteus vulgaris are the two leading causes of urinary tract infections and both are motile by means of flagella. Bacteria in the urinary tract tend to be washed out by the flow of urine. If the bacteria are able to move up the urethra, they are able to resist being flushed out. - capsules: A slimy layer of capsular polysaccharides protects bacteria from phagocytosis by masking surface antigens and reducing the attachment of antibodies. Capsules also help the bacteria to stick to surfaces and to form a biofilm. - adhesins: An adhesin is a protein that is found on the surface of a bacterium that helps it to stick to something. Some adhesins help bacteria to stick to specific sites on the surface of host cells. Bacteria that invade the gastrointestinal tract often have well developed adhesins that allow them to avoid being flushed away. (Sorry about the bad pun.)
Examples of Bacterial Virulence Factors and How They Increase Disease (cont.) - extracellular enzymes: Many pathogenic bacteria excrete digestive enzymes that break down parts of the host's defenses and body structures. This can allow the bacteria to penetrate deeper into the host's tissues or it can free up nutrients that the bacteria can utilize to grow. Example: Helicobacter pylori excretes mucinase, this enzyme degrades mucous in the stomach and allows the bacteria to penetrate to the tissues of the stomach wall where they cause ulcers. - toxins: A toxin is a poison that is produced by a microorganism. Toxins may harm tissues or trigger a pathological immune response. Examples of Bacterial Toxins: Cholera toxin made by Vibrio cholera causes severe diarrhea. Staphylococcus aureusmakes a heat stableenterotoxin that causes severe diarrhea and vomiting. (a form of food poisoning) Clostridium perfringens makes tissue necrosis factorwhich causes cell death in gangrene.
Examples of Bacterial Virulence Factors and How They Increase Disease (cont.) - antiphagocytic chemicals: Leukocidins are exotoxins that kill white blood cells (leukocytes) this is very bad because the white blood cells help fight the infection. - fimbrae or pili: Hair-like projections that help bacteria to stick to each other and to surfaces. Sometimes fimbrae have adhesion proteins as part of their structure. For more information, see chapter 14 in your text book. Information about adhesins is found on page 413, extracellular enzymes on page 418, toxins on page 418 and capsules on page 420. Some good examples of extracellular enzymes discussed in the text are: hyaluronidase, coagulase and streptokinase.
Bacterial Exotoxins & Endotoxins - An exotoxin is excreted by a bacterium. - Most exotoxins are proteins and many exotoxins are enzymes. - Exotoxins tend to target specific functions in the host. - An endotoxin is part of the bacterial cell or cell wall that elicits an inflammatory response in the host. - Endotoxins are released by growing bacterial cells as the debris of cell division or by bacterial cells that are decomposing. - Endotoxins tend to have a more general or systemic mode of action. - Lipopolysaccharide (LPS) from the outer membrane of Gram negative bacteria is the most common type of endotoxin. - LPS is a non-specific activator of the inflammatory response and a pyrogen (it causes fever).
Examples of Bacterial Exotoxins Diphtheria Toxin is an A-B type toxin - Diphtheria toxin is excreted by Corynebacterium diphtheria when it infects the throat. - Diphtheria toxin enters a host cell and acts as an enzyme that inactivates the host cell's ribosomes. Because the toxin is an enzyme, one molecule of toxin inactivates thousands of ribosomes, killing the host cell by shutting down protein synthesis. - In cases of diphtheria the bacteria rarely enters the host beyond an infection of the throat. But the toxin can travel through the blood and kill cells that are far away from the throat. If too many muscle cells in the heart are killed by the toxin, the patient dies.
Examples of Bacterial Exotoxins (cont.) Botulism toxin is excreted by Clostridium botulinum and is a neurotoxin that causes flaccid paralysis (muscles relax). Flaccid paralysis of the heart and lungs can be fatal. In food poisoning cases the bacteria produce the toxin while growing anaerobically in canned food. Ingestion of toxin causes disease without an infection. Tetanus toxin is excreted by Clostridium tetani and is a neurotoxin that causes rigid paralysis (muscle spasms). Tetanus kills the victim by exhaustion from constant muscle contraction. The toxin is produced by the bacteria when they infect a wound. Both of these Clostridial toxins are A-B type toxins. Streptococcus pyogenes hemolysin, an enzyme that damages cell membranes and can cause red blood cells to rupture. Staphylococcus aureus excretes a heat stable enterotoxin that causes severe nausea and diarrhea. Vibrio cholera toxin causes severe diarrhea. The gene for the toxin is encoded on a lysogenic bacteriophage. Strains of Vibrio cholera that don’t have the phage, don’t make toxin and don’t cause disease.
Infectious Disease TransmissionCommunicable DiseasesThe pathogen can be passed from person to person. - Typhoid fever (Salmonella typhi) a fecal-oral cycle pathogen - Typhus (Rickettsia prowazekii) transmitted by body lice - Tuberculosis (Mycobacterium tuberculosis) aerosol, coughing Noncommunicable DiseasesZoonoses (some) The pathogen’s normal host is an animal. - Rabies virus transmitted by animal bite/saliva - Woolsorter’s disease (cutaneous anthrax) Environmental Opportunistic Infections - Tetanus, Gangrene, Wound and Burn InfectionsAutoinfectionPathogen is a normal member of the body’s microflora.Bladder infection by E.coli
Epidemiology Epidemiology is the study of the interactions between disease causing pathogenic microorganisms and society. An epidemic is a sudden increase in the number of cases of a disease that are seen in a population. Tools of the Epidemiologist Include: - Statistics - Maps and Charts - Public Health Measures
Tools of the Epidemiologist Statistics - Prevalence : (total number of cases) / population Prevalence describes the health of a population in regards to a disease. - Incidence : (number of new cases) / population Incidence describes the rate of change in the number of cases. Prevalence is always a larger number than incidence because the total number of cases includes all new cases as well as old cases. For acute diseases with short durations, prevalence is closer to incidence and a decline in incidence is quickly followed by a decline in prevalence. For a chronic illness that has a long duration, prevalence may be substantially higher than incidence and a decline in incidence is not followed by a quick decline in prevalence. Incidence is a more predictive tool.
Public Health Measures - Mandatory Disease Reporting - Quarantine – Isolation of persons with an infectious illness - Enforcement of hygiene standards, especially in public eating places - Laws regarding clean water and sewage treatment - Mandatory Immunization – school enrollment requirements - In home assistance to persons with communicable diseases – TB officer
MCB 100 INTRODUCTORY MICROBIOLOGY Chapters 15 and 16 Host Defenses Against Infections
Chapter 15 Nonspecific Host Defenses Resistance and Immunity Resistance is the natural ability of a host to resist an infection by a microorganism that the host has never encountered before. Resistance relies on nonspecific defenses. Chapter 16 Specific Immunity Immunity is an enhanced resistance to a specific infectious agent that arises in a host as a result of previous exposure to that infectious agent. The immune response involves the production of specific proteins called antibodies that target defense responses against the specific pathogen.
Host Defenses Against Pathogens physical and chemical barriers on the surface of the body Resistance see: Chapter 15 defenses that are found inside the body that can inhibit or kill a microorganism that the host has never before encountered Immunity See Chapter 16 A specific immune response is not active until after the host has encountered a pathogen.
Three Lines of Defense Against Infections 1st Line (physical or chemical barriers) Skin, Mucous Membranes, Lysozyme (an enzyme found in tears and egg white that degrades bacterial and fungal cell walls) and Defensins (small antimicrobial proteins that are found in saliva, tears, sweat, and sebum) 2nd Line (inside the body, always present) Lactoferrin, Mononuclear Phagocytes, a-Interferon, Complement when it is activated by the Alternative or Properidin pathway, Inflammatory Response 3rd Line (specific immunity) Antibodies (made by B-lymphocytes), Cytotoxic T-Cells, Complement when it is activated by the Classical or Antibody-Dependant pathway.
Conditions that can cause a persons resistance to disease to be reduced: - old age - very young age - starvation - heredity - climate - poverty - stress - cuts and open sores Neonate - hospitalization - AIDS - cancer - immunosuppressant drugs Refugee camp - surgery
Nonspecific Resistance – The First Line of Defense Against Infection Physical and Chemical Barriers 1) skin: a physical and mechanical barrier, skin also provides some chemical barriers against microbial infection - enzymes in sweat degrade bacterial cell walls - defensins: small antimicrobial peptides - organic acids lower the pH - high levels of salt are caused by the evaporation of sweat (These factors inhibit microbial growth. Microorganisms that survive well on the skin as normal flora are usually not well adapted to infect deeper tissues.) 2) respiratory tract: Upper respiratory tract is lined with mucosal epithelium. This type of tissue produces a sticky substance called mucous that can trap microorganisms and also contains a lot of antibodies. The mucosal epithelium is also covered with tiny hair-like projections called cilia that move the bacteria that get trapped in the mucous towards the digestive tract.
The Body's Second Line of Defense Against Infection Phagocytes - A phagocyte is a cell that can engulf and devour microorganisms. They move around in the body searching for foreign objects like bacteria, that they eat. - Phagocytes play a role in resistance in that they can recognize and destroy invading bacteria in a nonspecific way. - Phagocytes also play a role in immunity when they work with antibodies to destroy specific bacteria. (Opsin independent phagocytosis occurs when a phagocyte binds to a bacterium because it has a receptor protein on its surface that sticks to a specific protein found on the surface of the bacterium. Opsin-dependent phagocytosis occurs when a phagocyte binds to and engulfs a bacterium that is coated with specific antibodies.)
Leukocytes and Phagocytes Leukocyte: Leuko = white, -cyte = cell, leukocytes are white blood cells Leukocytes are a major player in the body’s defense against infection. There are many types of leukocytes but two major categories: - lymphocytes: nonphagocytic, involved in specific immune responses - phagocytes: engulf and digest bacteria, yeasts and small protozoa Major Types of Phagocytes: - Monocytes: leukocytes with a large round nucleus that develop into macrophages - Macrophages: found in various parts of the body, such as the blood, lymph nodes, epithelial layers, mucous membranes - Dendrite Cells: found in intestinal walls, the thymus and other places - Kupffer Cells: macrophages in the liver - Microglial Cells: macrophages that are seen in the brain - Neutrophils: most common polymorphonuclear leukocyte (PMN)
Phagocytic cells have a greater affinity for bacteria that are coated with antibodies. (antibody production is a specific immune response) The coating of an infectious microorganism with a substance that increases phagocytosis is called opsonization. (opson = Greek, for sauce) Antibody function is covered on pages 467 – 468 of your text book, especially look at figure 16.6.
Inflammation - A General Response to Tissue Damage Inflammation is a big part of nonspecific resistance to infection because tissue damage is often caused by an infection or a wound. A wound provides a portal of entry for infectious microorganisms. Either way tissue damage is often correlated with infection. Four signs of inflammation: redness, swelling, heat and pain. - In inflammation, blood flow to the damaged tissue is increased. This causes redness and increases the traffic of nutrients and white blood cells to the damaged tissues. - Leukocytes & fluids leave blood vessels & move into damaged tissue causing swelling. - Phagocytes in the area of damaged tissue become activated. Activated phagocytes move more and synthesize antibacterial compounds. This increased metabolism produces extra heat. - Swelling and heat irritates nerves and causes pain.
The Body's Second Line of Defense Against Infection Complement - The complement system is a group of about 20 different proteins found in blood serum that play a role in destroying infectious microorganisms. - Some complement proteins bind to bacteria and other microorganisms and act as opsonins, others are cytokines or chemotactic factors and some form the membrane attack complex. - Complement proteins circulate in the blood in an inactive form and are activated by enzymes that cleave off blocking groups. Contact with bacterial endotoxin (LPS) or certain bacterial glycoproteins can cause the activation of complement factors. - Complement proteins can also be activated by antibodies. Antibodies are part of a specific immune response to a previously encountered pathogen. As such the complement proteins can play a part in both non-specific resistance to infection and specific immunity to a pathogen.
Activation of Complement Proteins (Alternative Pathway) The complement cascade is a series of enzymatic reactions involving the activation of complement proteins by proteolytic cleavage to remove blocking groups. When the final complement proteins are activated, they form the membrane attack complex, which can put holes in the cytoplasmic membrane of a pathogenic microorganism or an infected human cell.
Chapter 16 Specific Defense - The Immune Response Immunity is an acquired or enhanced resistance to infection by a specific bacteria or another microorganism. Immunity develops after exposure to the parasite. The result of an immune response is that the host synthesizes antibodies that bind to and attack that specific parasite.
Chapter 16 Specific Defense - The Immune Response Antigens An antigen is a foreign (non-self) complex which, when introduced into a host, causes the host to make specific antibodies that can bind to that antigen. Good antigens tend to be large molecules, such as proteins and protein-nucleic acid complexes. A good antigen needs to have two properties: immunogenicity (stimulates antibody production), and reactivity (binds effectively to an antibody). Antigens can be either soluble (such as a foreign enzyme, toxin or protein) or they can be particulate (such as a glycoprotein on the surface of a cell or an aggregate of molecules such as a flagella). Example: Influenza virus is covered by an envelope derived from a human cell membrane. Lipid is not a good antigen. There are two virus proteins that protrude from the envelope that are good antigens: Hemagglutinin and Neuraminadase (H and N). Strains of the influenza virus are classified by these antigens, such as H1N1 vs. H2N3 vs. H5N2 etc. Information about antigens can be found in the textbook, pages 462 – 463.
Chapter 16 Specific Defense - The Immune Response Antibodies An antibody is a protein that is found in blood serum or mucous that is formed in the host in response to exposure to an antigen. Antibodies are also called immunoglobulins. Antibodies are Y-shaped molecules that have two sites where the antibody binds to the antigen. The human body can produce millions of different types of antibody that differ from each other in the exact structure of the antigen binding sites. Each type of antibody is able to bind to only one specific type of antigen. The body can not produce all of the different types of antibody simultaneously because there is a limit to the amount of protein that can be dissolved in blood serum. A given specific type of antibody is only produced when the host has actually encountered the antigen that will bind to that particular antibody. Information about antibodies is in your textbook on pages 468 – 471.
Complement Activation (classical pathway – antibody mediated) - Specific antibodies attach to antigens on the surface of a bacterium or other microorganism. - The constant portion of the antibodies reacts with complement proteins 1, 2 and 4 to form a complex that activates complement proteins 3 and 5. - Activated C3 and C5 cause the other complement proteins to be activated (C6, C7 C8 and C9) and to form the membrane attack complexes (MAC). The MAC forms a circular hole in the membrane of the targeted cell. See figures 15.10, 15.11, 15.12
ANTIBODIES (immunoglobulins) An effective antibody will bind to an antigen and neutralize it.There are several ways that the binding of an antibody can inactivate the antigen. Antitoxins are antibodies that stop toxin molecules from damaging the host. An antiserum against a snake venom or bacterial toxin works like this. Antibodies can block the ability of a virus to bind to a host cell. Some antibodies act as opsonins, increasing the activity of phagocytic cells especially neutrophils (PMNs).
The following slides over some material from chapter 16 may help you with a couple of the LON-CAPA problems in Homework Folder 10.
Natural Immunity VS. Artificial Immunity Natural immunity occurs when a host encounters an infectious microorganism or an antigen is an uncontrolled fashion. Artificial immunity occurs when a host is deliberately exposed to an antigen for the purpose of producing an immune response. Active Immunity VS. Passive Immunity Active immunity is when a host produces antibodies that bind to and inactivate an antigen. In an active immune response an immunological memory develops. It takes a week and a half to two weeks for an active immune response to develop. Passive immunity is when a host receives preformed antibodies that were made by another individual. The recipient of the antibodies gains immediate protection from the antigen but does not develop an immunological memory.