Download
1 / 27
270 likes | 283 Views
Syphilis is still with us Paul R. Earl Facultad de Ciencias Biológicas Universidad Autónoma de Nuevo León San Nicolás, NL, Mexico.

E N D
Syphilis is still with usPaul R. EarlFacultad de Ciencias BiológicasUniversidad Autónoma de Nuevo LeónSan Nicolás, NL, Mexico
Syphilis is caused by the 5-15 micron spiral spirochete Treponema pallidum and is sexually transmitted. The bacterium spreads from the initial ulcer or chancre (shanker) of an infected person to the skin or mucous membranes of the genital area, mouth or anus of an uninfected sexual partner. In addition, a pregnant woman with syphilis can pass it to her unborn child, who may be born with serious mental and physical problems as a result of this infection: congenital syphilis.
Primary syphilis involves chancre and regional lymphadenitis. Secondary syphilis usually involves generalized rash, mucous patches and condylomata lata. These 2 stages last about 12-20 weeks and then syphilis becomes latent. During the first 2 years, the disease is called early syphilis.Pregnant women in hospital for maternity should be screened for syphilis, so that the result can be made available while they are still confined, and treatment can be provided if a positive diagnosis (seroreactive) is made. Their newborn infants should never be discharged from care until the mother's syphilis status is known.
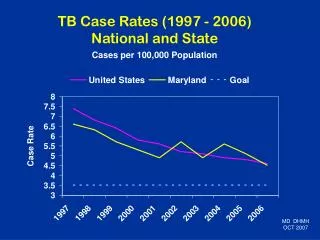
Primary and secondary syphilis rates*, by year - US, 1970-1997
HEALTH MINIMUMS INCLUDE:·Appropriate antibiotic therapy such as penicillin G·Careful screening for other sexually-transmitted diseases (STD) ·Referral of partner(s) to a sexual health service for diagnosis, treatment and contact-tracing ·Instructions to refrain from sexual activity during treatment ·Regular follow up of immunological testing to ensure that titers steadily decline to low levels
Elimination plans for sexualy transmissable diseases (STDs) have at least 5 strategies:- Increase surveillance. - Strengthen community involvement and partnerships. - Rapidly respond to outbreaks. - Improve and increase health promotion. - Expand clinical and laboratory services.
IS THERE A HAPPY ENDING TO THE SYPHILIS STORY ? WILL NORWAY, CANADA AND THE US BECOME MILESTONES ON THE ROAD TOGLOBAL ERADICATION?
Discovery“Everything” happened mostly in Germany from 1905 to 1910 !With a short life of 35 years, Fritz Schaudinn (1871-1906) and Paul E. Hoffmann (1868-1959) discovered Treponema pallidum in serumin 1905. Paul Ehrlich, father of immunochemistry and his assistent Hati. Fritz Schaudinn
In 1903, Elie Metchnikoff (1849-1916) and Pierre Roux (1853-1937) found that syphilus can be transferred from man to chimpanzee and from one chimpanzee to another.
In 1905, Aldo Castellani (1878-1971) discovered tropical yaws in children. August von Wassermann (1866-1925) and coworker Albert Neisser (1855-1916) devised a complement fixation test in 1906, and Paul Ehrich (1854-1915) found a cure in 1909. The arsenical Salvarsan, the magic bullet, worked. Metchnikoff shared the Nobel prize with Ehrlich in 1905.
The social past Europe learned about syphilis from Christopher Columbus (Cristóbal Colon) in the 16th century. By the 19th century it was riddled with syphilis from King Henry the 8th and his sterile wives and lovers, to the writers Edgar Allan Poe, Oscar Wilde and Guy Demaupassant, to painters Paul Gauguin and Vincent VanGough, through to the composers Ludwig von Beethoven and Robert Schumann. Insanity, tales of terror and bizarre acts connected these men. Once infected, the victim was infected for life before Salvarsan and more pointedly before penicillin by 1946.
Syphilis was used by feminists in fictional form in the 'New Woman' novels of the 1890s and earlier in England. These revolutionary novels for their day dealt with the burning issues of the women's movement such as marriage and motherhood. Do these novels—in any way—relate to the AIDS TV novels in South Africa?The corruption at the heart of highly desirable marriage was central to feminist novelists' messages. Syphilis in these novels acts as a powerful metaphor for the dangers to which unknowing women were exposed when pursuing what they were told should be their prime aim: a good marriage.
The New Women writers proposed that if a woman was informed of what to look for, she could protect herself against the predatory male with or without disease. Dorian Gray by Oscar Wilde is characterized as that syphilitic man, although of course never explicitly admitted for Dorian or Oscar. The Ladies's National Association for the Repeal of the Contagious Diseases Acts came forth against the assumptions on male sexuality and female guilt which underlay those Acts that punished women under the banner of medical necessity while ignoring the role of men, at least in the 1860s.
ProgressIs syphilis now replaced by AIDS? Of course, not. What is new and different? Antibiotics for one. Antibiotics on the one hand have radically reduced infant and child mortality, while on the other AIDS has raised it. AIDS is in the no-cure position syphilis was in for centuries. Still, untreated syphilis is also sometimes selfcures. We must ask: Why is syphilis not eradicated? Even when the technology is effective, it may not be taken proper advantage of. Lack of determination or plain ignorance can cause failure to eradicate both of these diseases and all the other STDs as well.
Many knowlegable communities or counties not paying the mandatory public health cost believe that they can sleep through epidemics that are well hidden. Again: If the public does not feel the threat, it will not demand the protection. Those not at risk, as always, do not want to pay taxes for diseases that do not concern them, except for the altruistic ultrarich. Does it follow these assertions that syphilitic rates are much higher in blacks than in whites? Yes. Is less public health money in poor districts? Yes. How does poverty relate to syphilis?
SYMPTOMSPrimary syphilisThe first symptom of primary syphilis is an ulcer called a chancre. It can appear within 10 days to 3 months after exposure generally appearing within 2-6 weeks. However as it is painless, the infected person might not notice it. It usually is found on the part of the body exposed to the infected partner's ulcer, such as the penis, vulva or vagina. A chancre also can develop on the cervix, tongue, lips or other parts of the body. It disappears within a few weeks treated or not. If not treated during the primary stage, about 1/3 of people will go on to the chronic stages.
Secondary syphilisA skin rash as in the illustration or with brown sores, often marks this chronic stage. The rash appears anywhere from 3-6 weeks after the chancre appears. The rash may cover the whole or part of the body and is almost always on the palms of the hands and soles of the feet.Since active spirochetes are present in such sores, any physical contact—sexual or nonsexual—with the broken skin of an infected person may spread the infection at this stage. The rash heals within several weeks or months.
Latent syphilisIf untreated, syphilis may enter the latent stage when no longer contagious and no symptoms are present. Many people who are not treated will suffer from no further signs and symptoms of the disease.Tertiary syphilisAbout 1/3 of people who have had secondary syphilis go on to develop the complications of late, or tertiary syphilis, in which the bacteria damage the heart, eyes, brain, nervous system, bones, joints, or almost any other part of the body. This stage can last for years, or even for decades.
NeurosyphilisYears after infection, neurosyphilis can be permanent, progressively destructive and life threatening, occurring in 4 forms: 1/asymptomatic, 2/ meningovascular, 3/ tabes dorsalis and 4/ general paresis of the insane. In meningovascular neurosyphilis, cranial nerve palsies and pupil abnormalities may be among a wide variety of symptoms. This may also cause damage to blood vessels resulting in stroke. In tabes dorsalis, progressive degeneration of the spinal cord occurs causing lameness. In general paresis, paralysis, tremors, seizures and mental deterioration occur as a result of damage to brain cells.
DIRECT SMEARSDarkfield microscopyDarkfield microscopy is used to demonstrate Treponema pallidum in material from lesions or lymph nodes. The presence of T. pallidum constitutes a definitive diagnosis of syphilis. Since T. pallidum is identified by characteristic spiral morphology and its motility, the preparation must be fresh and the organisms actively motile. Direct fluorescent antibody (DFA-TP)As an alternative to darkfield microscopy, fixed smears from lesions, serous fluid or lymph node aspirates may be sent to reference laboratories for staining with fluorescein-conjugated antibody to T. pallidum.
SEROLOGICAL TESTSNontreponemal or reagin testsThis group of common nontreponemal tests initiated by the Wassermann test measure antibody to a nonspecific cardiolipin lecithin antigen. The tests are moderately specific for syphilis (false-positives occur often), but highly sensitive.Because they are easilyperformed, the nontreponemal tests are useful screening tools. The tests can be quantitated to obtain a titer and, thus, are useful in monitoring patient response to therapy.
Treponemal TestsPrologue now! Treponemas can be cultured with mammalian cells (Infect. Immun. 32: 908–915, 1981 &36: 437–439, 1982), but most grievously such cultivation is little studied. Tissue culture (cell culture) could be a prominent source of antigens. Vaccine development is NOT a motive, because the risk is very low. Titration of antitreponema effects in vitro, cheaper than in rabbits is a challenge. The titration of antibiotics and other drugs is the MOTIVE for developing cultures.
TreatmentIf the patient has a reactive RPR or VDRL, a nonreactive confirmatory test,such as fluorescent treponemal antibody absorption (FTA-ABS),microhemagglutination assay for antibodies to Treponema pallidum (MHA-TP),or enzyme immunoassay (EIA), and no clinical or epidemiologic evidence ofsyphilis, no treatment is necessary. If clinical or serologic evidence of syphilis is found, or if diagnosis of syphilis cannot be excluded with reasonable certainty, the patient should be treated.
Intramuscular (IM) penicillin G is the drug of choice, despite some unfounded fears of resistant treponemal strains and possible anaphylaxis. Other applicable antibiotics are: a) Doxycycline 100 mg twice daily (BD) x 14 days, b) Erythromycin 500 mg 4 times daily (QDS) x 14 days, c) Azithromycin 500 mg daily x 10 days, d) IM Ceftriaxone 500mg daily x 10 days (if no anaphylaxis to penicillin), and e) Amoxycillin 500 mg 4 times daily plus Probenecid 500 mg 4 times daily x 14 days.
Is it true that for every doctor preferring parental therapy there’s a patient preferring oral therapy? The recommended IM penicillin G is the same as oral penicillin G and has 17 synonyms, e. g., ampicillin = amoxycillin. Many other medications, e. g., tetra-cycline, are effective against syphilis and others. Even though penicillen is supreme, perhaps one-dose in a cocktail that eliminates all bacterial STD agents is simple to attain. Or use—perhaps—just a FEW oral doses. Wake up America !
Some penicillin dosages are: primary, secondary and latent with a negative spinal fluid in adults and children over 12 years of age: 600,000 units daily for 8 days-total 4,800,000 units. Late (tertiary, neurosyphilis and latent syphilis with positive spinal fluid examination or no spinal fluid examination): 600,000 units daily for 10-15 days-total 6-9 million units. Congenital syphilis under 30 kg body weight: use 50,000 units/kg/day for 10 days.Has penicillin been adequately titered ?? No.