Download
1 / 33
330 likes | 338 Views
This case study explores the biopsy findings of a kidney transplant patient who experienced recurrent disease and chronic rejection. The biopsy results indicate borderline changes, probable chronic rejection with superimposed FK506 toxicity, and chronic transplant glomerulopathy. The Banff scores are provided for each biopsy.

E N D
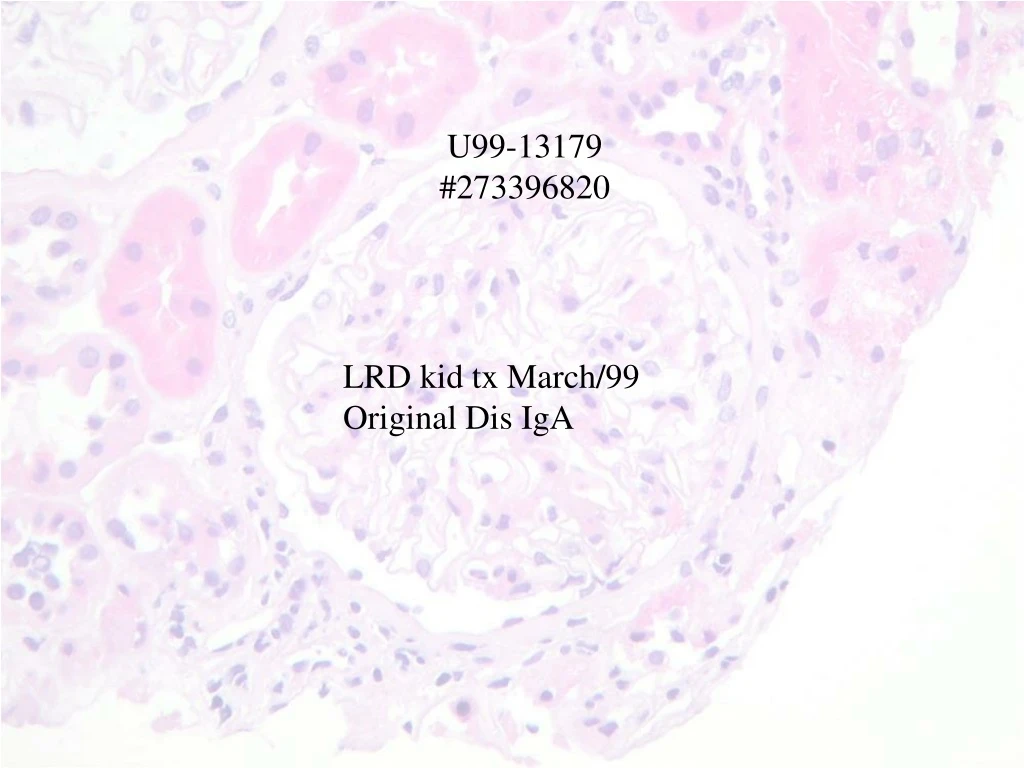
U99-13179 #273396820 LRD kid tx March/99 Original Dis IgA
U99-13179 DOB 26/5/67 1988 kidney biopsy with diagnosis Bergers IgA nephropathy 1997 September creatinine 500 1998 June creatinine 1300-urgent hemodialysis 1999 March start kidney transplant from sister Therapy: prednisone,Neoral,MMF/rad B25/ study Stable post transplant, creatinine 80-100 μmol/L Mild proteinuria and microscopic hematuria shortly after transplant 2002 increasing proteinuria to nephrotic syndrome with serum creatinine 120-180 range Avascular necrosis femoral heads :diagnosed 14/3/06 transplant biopsy: serum creatinine 250-300 protein/creatinine 25 serum albumin 42 On;prednisolone,Cellcept,Tacrolimus,Cozar,furosemide,Norvesc, acebutolol Is all clinical + biopsy change caused by recurrent disease?
IF • IgG- mild linear glomerular capillary(artifact?) • IgA- negative • IgM- trace mesangial-essentially negative • C3- moderate vascular and interstitial capillary • C1q-negative. • Kappa-mild linear glomerular,similar to IgG.Also moderate tubular droplet • Lambda-mild tubular droplet only • Fibrin- minimal interstitial • Albumin- strong tubular droplet and flat background
Diagnosis: Renal Biopsy: Borderline changes. No definitive evidence of rejection Rule out bacterial infection Banff score: (G1 CG0 I1 CT1 T1 CT1 V0 CV1 AH0 MM0)
U00-8893 #273396820 Renal transplant 18 months ago. increased creatinine prev bx 19 June rejection
IF • IgG: negative • IgA: negative • IgM: mild mesangial staining • C3: negative • C1q: negative • Kappa:negative • Lambda:negative • Fibrinogen: negative • Albumin:negative • C4d: Mild arteriolar staining.none in peritubular capillary
Diagnosis: Renal Biopsy: Probable chronic rejection with superimposed FK506 toxicity and acute tubular necrosis Banff score: (G0.CG1.I1,CT2,T1,CT2,V0,CV2,AH1,MM1)
Diagnosis: Renal Biopsy: Probable chronic rejection with superimposed FK506 toxicity and acute tubular necrosis. Banff score: (G0.CG1.I1,CT2,T1,CT2,V0,CV2,AH1,MM1)
U06-4991 #273396820 Original disease IgA LRD tx 1999. ↑creat 2000 with biopsy Proteinuria 2003 Creat now>200 but proteinuria gone?
IF • IgG- moderate to strong linear GBM staining • IgA- negative • IgM- trivial mesangial staining • C3- mild vascular staining • C1q-negative. • Kappa-moderate linear GBM staining • Lambda-negative • Fibrin- mild interstitial staining/mild glomerular staining • Albumin- minimal hyaline droplet change in tubular cytoplasm and mild linear GBM staining • C4d:No tissue left for C4d staining
Diagnosis: Renal Biopsy:(seven years post-transplantation) Chronic transplant glomerulopathy with 50% Glomerulosclrerosis Moderate parenchymal atrophy and scarring. Moderate hyaline arteriolar thickening suggesting calcinurine inhibitor toxicity. No evidence of acute rejection. Banff score: (G1 CG2 I1 CI2 T0 CT2 V0 CV1AH2 MM2)