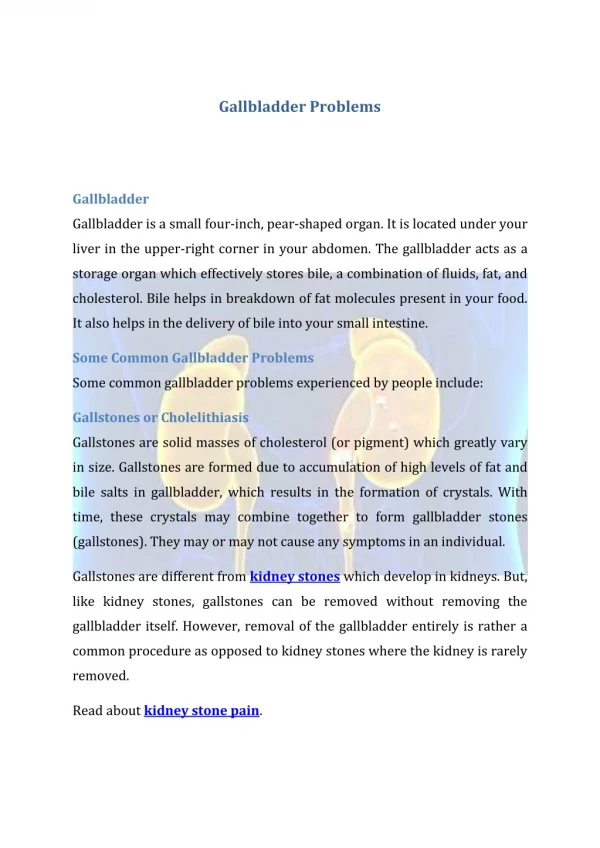
Download
1 / 16
190 likes | 796 Views
Joint Hospital Surgical Grand Round. Management of Gallbladder Carcinoma. Introduction. Fifth most common cancer in gastrointestinal tract More frequent in women Age standardized incidence rate ~3/100,000 in Hong Kong (including biliary tract cancer) 1

E N D
Joint Hospital Surgical Grand Round Management of Gallbladder Carcinoma
Introduction • Fifth most common cancer in gastrointestinal tract • More frequent in women • Age standardized incidence rate ~3/100,000 in Hong Kong (including biliary tract cancer)1 • Most preoperatively suspected cases are unresectable • Aggressive tumour biology • Multiple mechanisms of disease spread • Late presentation • Overall 5-year survival of 3-13%2 • Hospital Authority: Hong Kong Cancer Registry web site. www3.ha.org.hk/cancereg/e_stat.asp (accessed April 2012) • Jin K, Lan H, Zhu T, He K, Teng L. Gallbladder carcinoma incidentally encountered during laparoscopic cholecystectomy: how to deal with it. Clinical and Translational Oncology. 2011;13(1):25-33.
presentation • Incidental finding • Mimicking benign biliary tract diseases • 70% discovered incidentally by pathologist1 • 0.2-2.9% of all cholecystectomies2 • Late presentation • Biliary obstruction • Palpable mass / Hepatomegaly • Anorexia, weight loss • Malignant ascites • Goetze TO, Paolucci V. Immediate re-resection of T1 incidental gallbladder carcinomas: a survival analysis of the German Registry. Surgical endoscopy. 2008;22(11):2462-5. • ToyonagaT, Chijiiwa K, Nakano K, Noshiro H, Yamaouchi K, Sada M, Terasaka R, Konomi K, Nishikata F, Tanaka M. Completion radical surgery after cholecystectomy for accidentally undiagnosed gallbladder carcinoma. World J Surg. 2003;27(3):266-71.
Routine blood tests Ultrasound CT MRI (MRCP/MRA) investigations
Complete surgical removal of tumour is the only chance of cure • No truly effective chemotherapy or radiotherapy • Survival much higher if complete removal achieved during first resection • Treatment strategy depends heavily on staging Principle of management
Systematic review by SE Lee et al. (2011) No significant difference between simple or extended cholecystectomy in terms of survival Lymph node metastasis 1.8% Recurrence rate 1.1% Most studies showed 5-year survival rate >90% T1a (invades lamina propria)
T1b (invades muscular layer) • Simple cholecystectomy • 5-year survival rate of over 80% irrespective of surgical procedure1 • 10-year survival also comparable to extended cholecystectomy3 • Extended cholecystectomy • Frequent lymph node metastasis 1 for T1b(11% in T1b VS 2% in T1a; p <0.01) • Some studies showed significantly higher 5-year survival rate 2(79% VS 42%; p = 0.03) • Lower rate of recurrence 1(12.5% VS 2.7%; p <0.01) • Lee SE, Jang J-Y, Lim C-S, Kang MJ, Kim S-W. Systematic review on the surgical treatment for T1 gallbladder cancer. World journal of gastroenterology : WJG. 2011;17(2):174-80. • Goetze, T. O., & Paolucci, V. Immediate re-resection of T1 incidental gallbladder carcinomas: a survival analysis of the German Registry. Surgical endoscopy. 2008;22(11), 2462-5. • Wakai T, Shirai Y, Yokoyama N et al. Early gallbladder carcinoma does not warrant radical resection. Br J Surg 2001;88:675-8.
Extended cholecystectomy Extent of operation • Regional lymph node dissection • Liver resection • Wedge resection of liver bed • Variable resection margin • Formal segment IVb/V resection • Right hepatectomy / extended right hepatectomy • No consensus on extent of liver resection • Morbidity 28%; Mortality 1.5%1 • Lee SE, Jang J-Y, Lim C-S, Kang MJ, Kim S-W. Systematic review on the surgical treatment for T1 gallbladder cancer. World journal of gastroenterology : WJG. 2011;17(2):174-80.
T2 (perimuscular connective tissue) • Radical resection • Liver resection • Regional lymph node dissection • 5-year survival of1 • Simple cholecystectomy 10-61% • Radical resection 54-100% • Jin K, Lan H, Zhu T, He K, Teng L. Gallbladder carcinoma incidentally encountered during laparoscopic cholecystectomy: how to deal with it. Clinical and Translational Oncology. 2011;13(1):25-33.
T3 and T4 (beyond serosa / into liver) • Long-term benefit of aggressive surgery unclear • Aggressive resection only considered if potentially curative resection is feasible • 5-year survival 0-32%1 after radical surgery • Consider palliative care +/- metallic stenting if tumour not resectable • Jin K, Lan H, Zhu T, He K, Teng L. Gallbladder carcinoma incidentally encountered during laparoscopic cholecystectomy: how to deal with it. Clinical and Translational Oncology. 2011;13(1):25-33.
Lymph node dissection • T1b →N12 • T2/above → N1&2 • Significantly lower survival for node positive disease (5-year survival, 58–77% vs. 0–45%) • Curley SA. The Gallbladder. In: Bast RC Jr, Kufe DW, Pollock RE, et al., editors. Holland-Frei Cancer Medicine. 5th edition. Hamilton (ON): BC Decker; 2000 • Lai CHE, Lau WY. Gallbladder cancer--a comprehensive review. The surgeon : journal of the Royal Colleges of Surgeons of Edinburgh and Ireland. 2008;6(2):101-10. Available at: http://www.ncbi.nlm.nih.gov/pubmed/18488776. N1 N2
Pre-operative diagnosis Curley SA. The Gallbladder. In: Bast RC Jr, Kufe DW, Pollock RE, et al., editors. Holland-Frei Cancer Medicine. 5th edition. Hamilton (ON): BC Decker; 2000.
Intra-operative diagnosis Jin K, Lan H, Zhu T, He K, Teng L. Gallbladder carcinoma incidentally encountered during laparoscopic cholecystectomy: how to deal with it. Clinical and Translational Oncology. 2011;13(1):25-33.
post-operative diagnosis Jin K, Lan H, Zhu T, He K, Teng L. Gallbladder carcinoma incidentally encountered during laparoscopic cholecystectomy: how to deal with it. Clinical and Translational Oncology. 2011;13(1):25-33.
Aim at complete resection of the tumour Individualized approach for different stage of disease and timing of diagnosis Ongoing debate about management of T1b cancers and extent of lymphadenectomy, liver resection for each stage summary