Download

1 / 18
210 likes | 483 Views
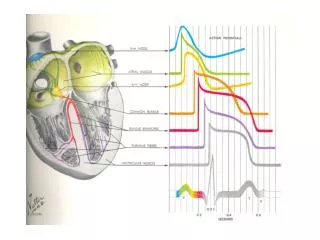
Supraventricular Tachycardias. Types: . SA source: Sinus tachy , SANRT Atrial source: EAT, MAT, AF, Aflut AV source: AVNRT , AVRT , JET. A-Flutter. Classical saw-tooth appearance on ECG .

E N D
Types: • SA source: Sinus tachy, SANRT • Atrial source: EAT, MAT, AF, Aflut • AV source: AVNRT, AVRT, JET
A-Flutter • Classical saw-tooth appearance on ECG. • Treatment/management essentially follows AF however flutter typically responds well to a low energy DC or to pace cardioversion • Often relatively insensitive to antiarrhythmic drugs.
Atrial Fibrillation • Most common sustained arrhythmias • Assoc. w/ ↑ CVS morbidity & mortality and preventable stroke. • CLASSIFICATIONS (3P’s) • Paroxysmal – self-ltd <24hrs • Persistant – recurrent >2days • Permanent – cardioversion unsuccessful
AF - prevention • ↓ incidence: ACE inhib, ARB’s & statins • Prevent after cardiac surgery with pre-op β-blockers, sotalol, amiodarone and statins
AF - causes • Cardiac: • IHD, cardiac failure, HTN, MI, PE, mitral valve Dz, CAD, ASD, cardiomyopathies, pericarditis, atrial myxoma, endocarditis. • Non- Cardiac: • Lung CA, pneumonia, hyperthyroidism, electrolyte imbalances, haemochromatosis, sarcoidosis, amyloidosis, phaeochromocytoma • Other: • Drugs, alcohol, caffeine • Lone AF • Familial
AF – from Hx • Details of palpitaions • Precipitating factors • Onset/offset • Nature • Duration • Assoc. Sx • Medications/drug use/alcohol/caffeine • Past medical Hx • Family Hx
AF – S&S • Can be asymptomatic • Chest pain • Palpitations • Dyspnoea • Dizziness • Irreg. irreg. pulse • Apical PR > radial PR
AF - Ix • Bloods: U&E, cardiac enzymes, thyroid fxn tests • ECHO: left atrial enlargement, MV dz, ↓ LV function any other abnormalities • CXR • ECG - later
AF - mangement 3 main objectives of treatment: • ID and treat causative factors (may abort arrhythmia) • Decide on rate or rhythm control (maintain sinus rhythm or control HR?) • Prevent thromboembolism – CHADS SCORE
Linear relationship btw CHADS2 score and risk of stroke with AF
CHADS2 scores, stroke risk, and risk levels CHADS2 scores, stroke risk, and risk levels
AF – acute mgmt <48hrs • If very unwell: O2, cardioversion, IV amiodarone • Tx assoc. illnesses • Control ventricular rate (1st choices: diltiazem, verapamil, metoprolol • Fully anti-coag: LMWH (keeps options open for cardioversion) • Cardioversion or drug cardioversion • For drug: amiodarone or flecainide
AF – long term mgmt • Rate or rhythm control? • RHYTHM: cardioversion (echo, pre-treat with Sotalol or amiodarone for >4wks if req.). Drug cardioversion. • RATE: Digoxin only in elderly sedentary. Others: atenolol, metroprololdiltiazem or verapamil are 1st line when there is failure to control exercise induced tachy. • Anti-coag – CHADS2. usually given atleast aspirin.
AF – Paroxysmal mgmt • Pill in pocket method often tried. • Sotalol or flecainide if infrequent, BP 100mg and no past LV dysfunction. • May also anticoag.
Absent P waves, erratic electrical activity instead. Irregularly irregular rate – no pattern Narrow QRS complexes ECG in AF - Absent P waves, erratic electrical activity instead. - Irregularly irregular rate – no pattern - Narrow QRS complexes