Download
1 / 18
180 likes | 494 Views
Delirium Assessment and Management. Presented by: Jonna Bobeck BSN, RN, CEN. Introduction. Acute change in consciousness Hyperactive delirium Hypoactive delirium Associated with increased length of stay Often goes undetected. Supporting Evidence. Need for standardized assessment tools

E N D
Delirium Assessment and Management Presented by: JonnaBobeck BSN, RN, CEN
Introduction • Acute change in consciousness • Hyperactive delirium • Hypoactive delirium • Associated with increased length of stay • Often goes undetected
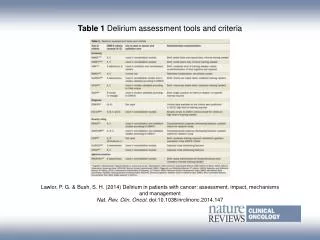
Supporting Evidence • Need for standardized assessment tools • Tools • Confusion Assessment Method (CAM-ICU) • Intensive Care Delirium Screening Checklist (ICDSC) • Also implementing the ABCDE bundle • A - awakening • B - breathing • C- coordination • C- choice • D - delirium
Supporting Evidence • Understudied and underreported • Pre-existing dementia, hypertension, alcoholism, and severity of illness • Recent studies conclude early mobility improves cognitive function • Decrease sedative use and modify iatrogenic risk factors
Managing ICU Delirium • The FDA has not approved a drug to treat delirium • FDA has issued an alert regarding antipsychotic medication • All patients receiving antipsychotic medications should be closely monitored
Managing ICU Delirium • Use the THINK mnemonic • T- toxic situations • H – hypoxemia • I – infection/sepsis • I – immobilization • K – electrolyte abnormalities
Delirium Screening • Patients admitted to Intermediate or Advanced ICU with be screened for delirium on admission and at least every 12 hours thereafter
Process for Utilization • Add the Delirium Screening to interventions • Complete the screening • Implement the ABCDE bundle
Process for Utilization: Patient Positive for Delirium • Orientation • Environment • Clinical paramaters
Process for Utilization: Patient Positive for Delirium • Pharmacologic • Use THINK mnemonic • T – toxic situations • H – hypoxemia • I – infection/sepsis • N – non-phamrocologic interventions • K – postassium or electrolyte problem
Early Mobilization • Patients will be progressively ambulated and mobilized • Objective assessment every 12 hours
Process for Utilization • Step 1: baseline mobility • Passive ROM twice a day • Turn every 2 hours • Increase sensory stimulation during day • Allow rest at night • Involve families
Process for Utilization • Assess mobility progression criteria • Responds to verbal stimuli with eye opening • Oxygen demands are stable • No unstable fractures • No increased titration of vasopressors for 12 hours
Process for Utilization: Progressive Mobilization • Step 2: bed to chair position • Step 3: life to chair • Step 4: dangle on edge of bed • Step 5: transfer to chair • Step 6: standing at bedside • Step 7: ambulate at bedside
Process for Utilization • Assess tolerance of activity by: • Unexpected change in vs • Symptomatic decrease in SBP • Decrease in Scvo2 • Increase in FiO2 • Desaturation less than 90% • Ventilator dysyncrony • Sustained increase in secretions
Key Points • O2 may not be increased during mobilization • Notify provider if FiO2 does not return to baseline • RT may adjust ventilator to support increased requirements • Advance only 1 step per day
Summary: Putting it all Together • ABCDE bundle
References • Pullman Regional Hospital,(2012). Delirium screening protocol Retrieved from \\prhs5\groups\Policies and Procedures\Patient Care • Pullman Regional Hospital, (2012). Early mobilization of ventilator patients protocol Retrieved from \\prhs5\groups\Policies and Procedures\Patient Care