Download

1 / 55
550 likes | 735 Views
Does impaired metacognition contribute to schizophrenic delusions ? Joëlle Proust. Metarepresentation and metacognition workshop University of Oslo April 29, 2014. Outline. Introduction: Cases of delusions Impaired Metarepresentational ability ( Frith 1992)

E N D
Does impaired metacognition contribute to schizophrenic delusions ?Joëlle Proust Metarepresentation and metacognition workshop University of Oslo April 29, 2014
Outline Introduction: Cases of delusions • Impaired Metarepresentational ability (Frith 1992) • Impaired simulation (Daprati et al, 1997, Jeannerod and Pacherie, 2004) • Impaired metacognitive control and monitoring • Impaired metacognition Conclusion: remediation?
Delusions • A delusionis « a beliefheldwithstrong conviction despitesuperiorevidence to the contrary » • This definitionisfaulty for taking a delusion to bemerely a belief; itmayoftenconsist in a global change in one’sexperience of the world • The inflexibility of delusionsdistinguishesthemfrom (truth sensitive) belief states. • Alternative definition: «a set of persistent bizarre or irrationalbeliefsthat are not easilyunderstood in terms of an individual’s social or cultural background ». • Somedelusions are not caused by a mental illness, but rather by highfever, poisoning, drugs, hemiplegia etc.
Cases of delusion • Delusion of control of one’sactions • Delusion of reference • Thought insertion, thoughtwithdrawal, thoughtbroadcasting • Persecutorydelusion • Fregoli delusion • Erotomania • Cotardsyndrom • Grandiose & religiousdelusions • Proprioceptive delusion • Capgrasdelusion
Cases of delusion • Delusion of control of one’sactions • Thought insertion, thoughtwithdrawal, thoughtbroadcasting • Persecutorydelusion • Delusion of reference • Fregoli delusion • Erotomania • Cotardsyndrom • Grandiose & religiousdelusions • Proprioceptive delusion • Capgrasdelusion
Delusions of control Some patients with schizophrenia, as well as brain-lesioned patients with alien hand syndrome, present a dissociation between • the feeling that their own body is moving – an experience of ownership related to the fact that something is happening to the self, • the feeling that their body is being moved by a foreign intention, rather than of the subject’s own will – a perturbed feeling of agency.
4 intriguingfeatures • Asymmetrybetween SO and SA: no case of an impression of agencywithout an impression of ownership, no symmetricaldelusion. • Comparable xenopathy in delusion of control and thought insertion. • External attribution versus feeling of non-agency • Ocasionalityproblem: whyisagencyimpaired in certain cases not others?
Hypothesis 1: metarepresentation • A) The generation of intentions to act is massively impaired in patients: poverty of will, lack of persistence in their work, poor personal hygiene, difficulties communicating with others. • B) Intention control and monitoring is also often impaired: patients have difficulties selecting an appropriate action-schema • C) Finally, patients with schizophrenia monitor their actions in an abnormal way. They are able to correct failed actions only if they have access to visual feedback, in contrast to normal subjects, who also rely on internal forms of monitoring.
The control of action: Shallice (1988) Two functional levels • the contention scheduling system (CSS) activates effectors on the basis of environmental affordances and triggers routine actions. It is regulated by mutual inhibition ("winner takes all"). • the Supervisory Attentional System (SAS) is able to trigger non-routine actions, or actions that do not involve stimuli presently perceived.
The MR dimension • The main feature of SAS that allows it to both provide an agent with conscious access to her actions and to control routine actions is a metarepresentationalcapacity. • Frith (1992): If metarepresentation is malfunctioning, there will be an imbalance between higher-level conscious processes and lower-level unconscious processes. As a result, patients will be aware only of the contents of propositions, not of the metarepresentations in which they are embedded.
Frith 1992 • Having had metarepresentations in the past, they are still able to attempt to form them. But they end up grasping only the embedded content: • When trying to form the thought that someone thinks about P, they might only think P • Instead of considering some form of action/thought, they will mistake the representation of a possible action/thought for a command to act/think
Objection: overgeneralization • Patients don’t have trouble reportingtheirown mental states: they are « hyperreflexive » (Sass et al. 2001) • They are not impaired in readingminds in contexts not involving action of the self. • Does not explain attribution of own actions to others.
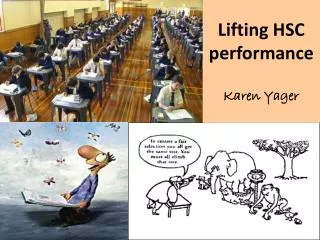
The motor control hypothesis: A faulty or irregularefference copy? • When acting, a forward model of the action is activated by the command. • A comparator cuts down the amount of feedback required to check whether the action is successful, and makes control of action in normal subjects smooth and quick. • In schizophrenia, the comparator might be faulty, thus depriving the agent both of the capacity to anticipate the observed feedback and to consciously take responsibility for her actions and thoughts (Feinberg (1978). Frith& Done,1989, Malenka et al., 1982; Mlakar, Jensterle,. & Frith, (1994), Wolpert et al., (1995); Blakemore, Rees, & Frith, (1998).
Predictor Forward model Predicted Sensory Feedback (Corollary Discharge) Efference Copy Sensory discrepancy Sensorimotor System Motor Command Actual Sensory Feedback Sensation
The motor control hypothesis: A faulty or irregularefference copy? • Patient with delusion of control is aware of • (i) her goal, • (ii) her intention to move, • (iii) her movement having occurred, • But not of (iv) her having initiated her movement, because she failed to predict the sensory consequences of the movement.. Frith& Done,1989, Malenka et al., 1982; Mlakar, Jensterle,. & Frith, (1994), Wolpert et al., (1995); Blakemore, Rees, & Frith, (1998).
the motor control system makes use of internal models, including inverse and predictive models, and comparators. • action-control mechanisms and action-awareness mechanisms are importantly connected. • Matching feedback correlates with a sense of agency for the action. • degree of mismatch between predicted and observed feedback modulates activation in the right inferior parietal lobule, and is responsible for external attributions of action.
the sense of extraneity result from a lack of sensory self-attenuation, itself caused by a failure to predict consequences of one’s own actions. (Blakemore et al., 2000: self-tickling & auditory hallucinations) • the sense of passivityresultsfrom the absence of self-attenuation
Question • How does a meredifficulty in predicting the consequences of one’s actions generates, on top of a perturbedsense of agency, an attribution to others of one’s actions, eventhough the sense of ownershipis not perturbed?
First attemptataddressing the problem: the simulation theory
Impaired simulation Simulation mechanisms are activated when observing as well as imagining and executing actions. Intentions to act are thus represented impersonally. • Such impersonal intentions are labelednaked intentions. • recognition of own/others’ agency depends on observed cues. Patients with schizophrenia have a general difficulty in simulating actions. Evidence from subjects with auditory hallucination suggests that they do not predict feedback from their own inner speech – another form of covert, simulatory activity. (Daprati et al, 1997, Jeannerod& Pacherie, 2004)
Impaired simulation: a who system involved • The motor system represents the actions of others to the sameextentthatitrepresentsagent’sown. • The phenomenology of alien control might result from impairments to the mechanisms controlling and/or monitoring the different modes of simulation involved in the ‘Who’ system. (Daprati et al, 1997, Jeannerod& Pacherie, 2004, Pacherie et al 2006)
Impaired simulation 2004 follow-up by Farrer et al. of Daprati et al.'s 1997 study shows that the level of activity in the patient’s right posterior parietal cortex fails to be proportional to the discordance between expected and observed feedback, as it is in control subjects. A defective simulation mechanism, rather than a defective action monitoring mechanism, combined with a general disruption of the self-other distinction, could be responsible for an impaired sense of agency in patients with schizophrenia. (Daprati et al, 1997, Jeannerod& Pacherie, 2004, Farrer et al. 2004)
Objections • If generally impaired simulation underlies the patients’ deficits, why do they seem to plan their actions normally? • why do patients with alien control delusions believe that particular agents are controlling their actions? • Is self-identity affected by impaired self-attribution of actions, and how so? • how does the view explain that attribution of action and thought are both impaired? • Occasionalityproblemunsolved • delusioninflexibility not explained
Second attemptataddressing the problem: the revised control theory Fletcher & Frith (2009)
Common mechanismhypothesis • Max Coltheart (2007) has arguedthat an account of delusions must include an account of impaired perception, and an account of abnormalbelief. • Against a two-deficitaccount, F & F (2009): • Theory of coincidental damage unlikely • Minimization of predictionerrorexplainsboth the hallucinatory aspect (abnormal perception) and the delusional aspect of perturbed SA in schizophrenia.
Abnormalconnectivity • Sensoryconsequences of self-generatedactsshouldnormallyelicitlessbrainactivitythanthose of an externallygeneratedact. • This is not the case in Schizophrenia: thereis a poorconnectivity • betweenmotor and sensoryregions(fMRI by Mechelli et al. 2007) • Between rostral and caudal LPFC regions (Barbalat et al. 2011) pb in « bindingdifferent temporal features of information into a temporary, unitary and coherentrepresentationwithin the episodic buffer » Fletcher & Frith (2009)
KoechlinSommerfield 2007lin
Functionalrole of system hierarchy • Predictionerroremitted by a lower-levelprovides input for a higher-level system (« input not fullyaccounted for ») • Feedback from the higher-level system issupposed to • provide a readjustement to reduce the predictionerror (new beliefs and inferences) • Motivatediscounting the present model • Reallocate attention: a violation of expectation renders an occurrence more salient (Kapur 2003) Fletcher & Frith (2009)
System hierarchyimpaired in schizophrenia • Predictionerrorsemitted by the lower- level system are false, hence • cannotbesolvedat a higher-level • Propagatehigher up: delusionalbeliefthatothers control self, changedself-identity, etc.
System hierarchyimpaired in schizophrenia • Predictionerrorsemitted by the lower- level system are false, hence • cannotbesolvedat a higher-level • Propagatehigher up: delusionalbeliefthatothers control self, changedself-identity, etc.
What is the contribution of Impaired metacognition to schizophrenic delusions?
Wheredoesmetacognitionstep in? • When a predictionerrorisoccurring, itdoes not need to bemonitored by metacognition (specialized in monitoring cognitive actions) • Acting, however, normallyelicitsin humans, noetic feelings, i.e. predictions about what one canremember, discriminate, understand, in brief: all the information thatcanbeexploited to achieve and furtherone’s goals. • It seemsthatthese feelings, in patients, tend to express eitherinflated or no confidence at all
Impairedmetacognition An impairedmetacognitioncanresult • Frominappropriate monitoring – failing to have uncertainty feelings/ judgmentsmatching the validity of the performance • Frominappropriate control – failing to use monitoring to make congruent control decisions.
Impairedmetacognition An impairedmetacognitioncanresult • Frominappropriate monitoring – failing to have uncertainty feelings/ judgmentsmatching the validity of the performance Garety • Frominappropriate control – failing to use monitoring to make congruent control decisions Koren
Noetic feelings • Have generally been ignored as a component in the hierarchical control systems Noetic feelings, however, are permanently monitoring the informational changes thatourbodily actions generate as a sideeffect. You recognize a face or a place as familiar, youfind a sign as strange, a landscape as beautiful, an activity as boring.
Frompredictionerror to metacognition • Phenomenasuch as enhancement of background sounds or sightsthatshouldbeirrelevantcanbeexplained by the predictionerrorbeinginappropriatelyquantifiedthroughinappropriatehigher-level top-down modulation. • Stimuli with large predictionerrorswillbe • felt as strangeand externallygenerated • Seen as demanding attention • More readily associable Fletcher and Frith 2009
Role of predictionerror in noetic feelings • Enhancedsensoryexperiences are a source of noetic feelings, becausetheyconstitute in themselves « epistemic affordances » • More salient more fluent • More relevant more motivating for attention , thinking and planning • More readilyassociable More informative Fletcher and Frith2009, Proust 2014
A powerful source of motivation • Clinicalevidencesuggeststhat patients are oftenverymotivated by the metacognitive feelings elicited by theirmodified perceptions and by theirpotential new status as cognitive agents. • Some of themevenseethemselves as about to build up far-reachingtheories about the universe, or about society, etc. • thispositivelyrewarding feedback fromnoetic feelings mightparticipate in fixing the delusion. (Pessiglione et al. 2006)
Dichotomousconfidence & monitoring • It is not the predictionerrors per se that are faulty, but the waythey are « quantified »: uncertainty about predictionerror and about itssignificance are poorlyestimated: • Undueweight to smallpredictionerror + underestimation of uncertainty = false inference • A large predictionerrormayberejected by being « diluted in excessive noise » Fletcher and Frith 2009
Whydichotomousconfidence ratings ? • There are twoways of understandingdichotomous confidence ratings: • Either as reflecting an impairment in monitoring one’s confidence • Or in reflecting an impairment in control sensitivity
dichotomous confidence & monitoring Reasoning biases are generally understood from poor monitoring • belief inflexibility: Delusional beliefs are felt by patients as self-evident • jumping to conclusions = restricted data gathering: • dichotomous confidence rating (all or nothing): « extremeresponses » Garety et al. (2005),
dichotomousconfidence: monitoring? Reasoning biases are generally understood from poor monitoring • belief inflexibility: Delusional beliefs are felt by patients as self-evident = might also be a problem of failing to revise a belief • jumping to conclusions = restricted data gathering is a problem of control not monitoring • dichotomous confidence rating (all or nothing): « extremeresponses »: alsopossibly a matter of control
Arguments in favor of a control problem • Belief inflexibility: People able to report alternative explanations for their delusional beliefs are more likely to respond positively to the possibility of being mistaken (Freeman at al., 2004). • Garety interprets as belonging to belief monitoring; • reflecting on one’s own beliefs, • changing them in the light of reflection and evidence, • generating and considering alternatives” Garety et al. (2005)
In Garety’s model, however, the crucial stepsinvolve control …/
Garety et al. 2005: reasoningprocesses in delusion conviction and change ER= extremeresponding JTC= jumping to conclusions PM= possibility of beingmistaken
Thinking style in delusions (Garety et al. 2005) • Jumping to conclusions (on a probabilisticreasoningtask) and more frequentendorsement of extremeresponsesindependentlyconribute to beliefinflexibility- misrecognition of possibilityof beingmistaken. • The jumping to conclusions bias is thought to reflect a data-gathering bias, specifically, the rapid acceptance of a proposition in the absence of much information (Garety & Freeman, 1999). • consistent with the hypothesis that patients make less use of past information when forming judgments and are overinfluenced by current stimuli at the expense of context or previous learning Hemsley, 1988; Kapur, 2003).
Dichotomous ratings and control • An alternative explanationisthat patients, due to an executivedifficulty in associating a decision to a particularcontext, fail to correctly translate their feeling of confidence with the correspondingdecision to respond, in particularwhenthisresponseisofferedverbally.
Impaired metacognitive control sensitivity 30 patients with first episode of schizophrenia. • Asked to perform a Wisconsin task sorting task • Then, asked to rate their level of confidence in the correctness of their performance • Finally, asked to choose whether they want this trial to be ‘‘counted’’ toward their overall performance score on the test. Koren et al., 2006
Koren et al.,2004 Results: Insight into illness was correlated with • correct confidence rating • adequate control sensitivity. • some patients, however, presented a dissociation between correct monitoring and inadequate control = failure in control sensitivity (correct subjective feedback, but not used in selecting action).