Download
1 / 19
200 likes | 461 Views
Tightrope Fixation for Syndesmosis Diastasis – What’s the Evidence?. Mark Porte, MD University of Toronto. Case. 39 YO active female External rotation injury to right lower extremity Fall with leg caught under her Unable to weight bear post injury On exam: Pain at syndesmosis.

E N D
Tightrope Fixation for Syndesmosis Diastasis – What’s the Evidence? Mark Porte, MD University of Toronto
Case • 39 YO active female • External rotation injury to right lower extremity • Fall with leg caught under her • Unable to weight bear post injury • On exam: • Pain at syndesmosis. • +ve squeeze test, +ve external rotation test
Follow-up – 3 Months • Rehab Protocol • Splinted 0-2 weeks • Aircast 2-6 weeks • NWB ROM exercises • Progressive WBAT at 6 weeks • At last f/u good ROM (details not documented) • Pain free weight bearing • Progressing back to regular activities
Tightrope – Theoretical Advantages • Preserve physiologic motion? • Reduce hardware pain? • Eliminate need for second surgery? • Earlier return to motion/activity?
Evidence? 4 Case Series • Walking a tightrope: Our experience in the treatment of traumatic ankle syndesmosis rupture • D. McMurray, B. Hornung, B. Venkateswaran, Z. Ati • Treatment of syndesmotic disruptions with the Arthrex Tightrope: A report of 25 cases • Cottom JM, Hyer CE, Philbin TM, Berlet GC • Outcome and complications of treatment of ankle diastasis with tightrope fixation • HJS Willmott, B. Singh, LA David • Treatment of syndesmosis disruptions with TightRope fixation • JC Coetzee, P Ebeling
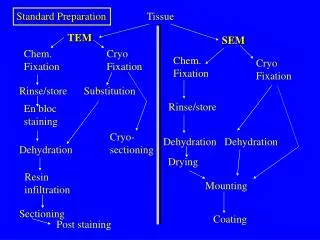
Klitzman R, Zhao H, Zhang LQ, Strohmeyer G, Vora A. Suture-button versus screw fixation of the syndesmosis: a biomechanical analysis. Foot Ankle Int 2010 Jan;1(1):69-74 • 8 cadavers, 3 groups • Intact ligaments • Syndesmosis repaired with screw • Syndesmosis repaired with tightrope • Construct cycled under submaximal loads • Syndesmotic gap less after loading (p=0.0004) in screw group compared to control and tightrope • Increased coronal (p=0.0002) and sagital (p=0.005) plane motion after cycling in tightrope group compared to control • Decreased coronal (p=0.00014) and sagital (p=0.0000012) plane motion after cycling in tightrope group compared to control • Study conclusions: Tightrope construct more closely mimicked physiologic syndesmotic motion
D. McMurray, B. Hornung, B. Venkateswaran, Z. Ati. Walking a tightrope: Our experience in the treatment of traumatic ankle syndesmosis rupture. Injury Extra 2008;39:182. • Prospective; sequential patients • 16 patients • All with associated fractures • Mean follow-up 5.5 months • Mean time to weight bearing 6 weeks • No re-displacement • 3 hardware removal (2 infection, 1 soft tissue irritation)
Cottom JM, Hyer CE, Philbin TM, Berlet GC. Treatment of syndesmotic disruptions with the Arthrex Tightrope: a report of 25 cases. Foot Ankle Int 2008 Aug;29(8)773-80. • Retrospective review of 25 cases over 2y. Single Hospital • Mean follow-up 10.8 months • 21 using single tightrope, 4 using double tight rope • Associated ankle fractures treated according to AO principles • Mean time to weight bearing 5.5wks • No evidence of re-displacement of syndesmosis • No cases of hardware removal • “Considered a good option”
Willmott HJS, Singh B, David LA. Outcome and complications of treatment of ankle diastasis with tightrope fixation. Int J Care Injured 2009;40:1204-5. • Retrospective review, single hospital • 6 cases met inclusion criterion • 5 cases associated with ankle fracture • Mean follow-up 6 months • Mean time to weight bearing 6 weeks • No evidence of re-displacement • 2 cases of hardware removal secondary to soft tissue irritation
Coetzee JC, Ebeling P. Treatment of syndesmosis disruptions with TightRope fixation. Techniques in Foot and Ankle Surgery. 2008;7(3):196-202. • Ongoing RCT • Average follow-up 18.5 months • 8 patients per group • AOFAS (Ankle an hindfoot score) 94 vs 88 • No evidence of syndesmotic loosening • 1 tightrope removal for soft tissue irritation • Trend toward increased ROM in tightrope group however screw not routinely removed
Conclusions • Limited literature • Appears to be a safe option • No published evidence for re-displacement • May necessitate tightrope removal (0-33%) • Better range of motion compared to intact in situ screw in biomechanical testing
Conclusions • Preserve physiologic motion? • Compared with intact syndesmosis screw. Most likely • Reduce hardware pain? • Maybe? • Eliminate need for second surgery? • Maybe? • Earlier return to motion/activity? • Doesn’t seem to be
Clinical Exam – The Classics 2. Squeeze test 1. syndesmotic pain 4. Fibular translation 3. External rotation test
Tenderness LengthIn the absence of diastasis Nussbaum et al (2001) • Length of tenderness measured from tip of lateral malleolus correlates with time to return to sport in sprains with no diastasis
Tenderness LengthIn the absence of diastasis Days Lost = 5 + [0.93xTL(cm)] +/- 3.7 Nussbaum et al (2001)
Manjoo A, Sanders DW, Tieszer C, MacLeod MD. Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma. 2010 Jan;24(1):2-6. • Retrospective review of 106 cases • 76 underwent formal testing (mean f/u 23 mo) • Outcomes: Lower Extremity Measure (LEM) and OlerudMolander score (OM) • Decreased functional outcome in patients with intact syndesmosis screws. (LEM, p=0.01; OM, p=0.04) • No functional difference between broken, loose or removed syndesmosis screws