Download

1 / 47
480 likes | 752 Views
PKOS’unda GnRH anolog vs. antagonist. Dr.Engin Oral İ.Ü. Cerrahpaşa Tıp Fakültesi Kadın Hastalıkları ve Doğum Anabilim Dalı Reprodüktif Endokrinoloji Bilim Dalı Tüp Bebek Ünitesi. Agonist. GnRH reseptörlerinde down regülasyon ve desensitizasyon. Antagonist.

E N D
PKOS’unda GnRH anolog vs. antagonist Dr.Engin Oral İ.Ü. Cerrahpaşa Tıp Fakültesi Kadın Hastalıkları ve Doğum Anabilim Dalı Reprodüktif Endokrinoloji Bilim Dalı Tüp Bebek Ünitesi
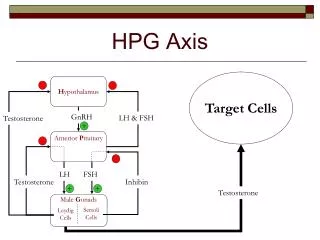
Agonist • GnRH reseptörlerinde down regülasyon ve desensitizasyon
Antagonist Hipofizer Gn reseptörlerinde kompetitif blokaj
Antagonist(Beklenen Avantajlar) • Flare-up etki yok • Hemen etki (FSH ve LH) • Süpresyon etkisi doz bağımlı • Östrojen eksikliği semptomları yok • Daha kısa tedavi süresi • Daha az gonadotropin kullanımı • Deri altı uygulama • Antagonist siklüslerinde ovulasyon tetiklemesi için agonistler kullanılabilir • Daha az OHSS • Daha az maliyet
GnRH ANTAGONİST İki İlaçİki protokol Ganirelix Multiple doz Antagon, Orgalutron (Organon) Lübeck Cetrorelix Cetrotide (Serono) Tek doz French
GnRH Antagonists Protocols 17-20mm 14 mm MENSTRUATION 36 h. DAY 1 2 3 4 5 6 7 8 FSH/HMG 75 UI HCG 10000 UI GnRH Antagonist 3 mg The single dose (French) protocol
GnRH Antagonists Protocols 17-20mm MENSTRUATION 36 h. DAY 1 2 3 4 5 6 7 FSH/HMG 75 UI HCG 10000 UI GnRH Antagonist 0.25 mg Multiple doses (Lubeck) daily protocol
Why is the clinical acceptance of gonadotropinreleasinghormone antagonist cotreatment duringovarian hyperstimulation for in vitro fertilization soslow? Bart C. J. M. Fauser, and Paul Devroey,2005
Agonist vs Antagonist Trials Cochrane study; Al-Inany, 2001 • 5 RCTs • 1796 women randomized -1211 antagonist -585 agonist Cochrane study; Al-Inany, 2006 • 27 RCTs • 3865 women randomized -2292 antagonist -1573 agonist
Description of Studies Twenty-seven RCTs were identified • twenty trials involved an unspecifed population of infertile couples • seven trials were performed in specific infertile populations. • 'poor responders' (Inza 2004;Cheung 2005; Marci 2005), • 'polycystic ovary syndrome‘ (Kim 2004;Bahceci 2005), • 'mild male factor' or 'unexplained infertility'(Zikopoulos 2005) and 'tubal factor' (Causio 2004).
Analysis done on the number of women randomised, not all on participants Individual trials Significant less FSH/HMG Significant shorter duration of stimulation No statistically significant pregnancy rate
Pregnancy per Women • Clinical pregnancy rate significantly lower in the antagonist group. (OR 0.84, 95% CI 0.72 to 0.97) in favor of the long GnRHa protocol. • Absolute treatment effect (ATE) 4.7% • Number needed to treat to benefit (NNTB) 21 • Ongoing pregnancy/ live birth rate significantly lower in the antagonist group. (P= 0.03; OR 0.82, 95% CI 0.69 to 0.98)
Incidence of Severe OHSS • Statistically significant reduction in incidence of severe OHSS with antagonist protocol. • The relative risk ratio was (P = 0.01; RR 0.61, 95% CI 0.42 to 0.89). • Interventions to prevent OHSS (e.g. coasting, cycle cancellation) were administered more frequently in the agonist group (P = 0.03; OR 0.44, 95% CI 0.21 to 0.93). • Risk difference was estimated to be -0.02 (95% CI -0.03 to 0.00).
Spontaneous miscarriage rate • No statistically significant difference between the two protocols regarding the incidence of multiple pregnancy and miscarriage rates • Similar between the two groups [(P = 0.31; OR 0.84, 95% CI 0.59 to 1.19) and (P = 0.83; OR 0.95, 95% CI 0.61 to 1.49)
GnRHa vs. Antagonist A systematic review and meta analysis The rate of live birth rate was 2.7% higher with agonists, but the difference included zero. Kolibianakis EM, 2006
Treatment Of The HyperresponderThe Goal • Increase follicular phase FSH levels • Decrease follicular phase LH levels • Decrease insulin and androgen levels • Minimize excessive E2 elevation • Increase proportion of mature sized follicles • Minimize the risk of OHSS
A meta-analysis of outcomes of conventional IVF in womenwith polycystic ovary syndrome E.M.E.W.Heijnen, 2006
Rationale for antagonists in PCOS • Ability to • Flexibly supress LH in the folicular phase • Avoid lengthy supression, as seen with agonists, in those at risk for low response • Use GnRH agonists to trigger ovulation in those at risk for OHSS • Potential use in minimal stimulation protocols
Can Antagonists Be the optimal choice for COH in PCOS • Must • Be ‘‘non inferior’’ to accepted protocols • Not increase the risk of OHSS • Result in equal patient tolerance • Be acceptably convenient to perform for both patient and physician
Cetrorelix 3 mg in PCOs Cetrorelix 3 mg Previous cycle N = 34 Long agonist N = 34 Stimulation duration 12.9 Total dose of rec-FSH 1921 325 E2 at day hCG 2077 754 3254 652 No of oocytes retrieved 13.4 6.1 18.2 5.9 No of mature oocytes 8.3 4.2 15.5 5.5 Pregnancy rate 35.2% Severe OHSS 1 (3%) 8 (23%) Cancellation of over-response 0% 38% (Avril et al 2002)
IVI : 1/7/2002 – 30/6/2003 1473 cycles / 1092 transfers 45,6 43,6 34,6 31,5 28,4 28,6 p = NS n = 705 / 535 n = 768 / 555
PCO p <0.01 Dr. José Navarro 64,9 35,1 41,1 22,3 52,9 22,8 n = 70/57 n = 57/37 2004
Reproductive outcome of polycystic ovarian syndrome patients treated with GnRH antagonists and Rec FSH for IVF/ICSI Kolibianakis E, 2003
A significantly lower ongoing pregnancy rate per oocyte retrieval and a higher occurence of OHSS was observed in the group of patients with BMI >29. Also in the BMI ≤29 group there is a tendency towards higher ongoing implantation rate and a lower miscarriage rate
The impact of using GnRH antagonist in COH for ART in women with PCOD: a randomized study • 70 pts in Agonist arm • 59 pts in Antagonist arm • No premature LH surge • Shorter duration in Antagonist arm • No difference in consumed • gonadotropins • 4. Similar OHSS incidence p>0.05 for both IR and PR Bahceci et al, 2005
Comparison of GnRH agonists and antagonists in assistedreproduction cycles of patients at high risk of ovarianhyperstimulation syndrome historical controls 18 pregnancies (20.7 per initiated cycle; 31.6% per embryo transfer) G.Ragni, 2005
Triggering final oocyte maturation using different dosesof human chorionic gonadotropin: a randomized pilotstudy in patients with polycystic ovary syndrome treatedwith gonadotropin-releasing hormone antagonistsand recombinant follicle-stimulating hormone • Eighty PCOS patients. • Patients were randomized to receive 10,000 IU (28), 5000 IU (26), or 2500 IU (26) ofhCG for triggering final oocyte maturation • The median fertilization rates were 52.8%, 65.4%, and 55.6% after administration of 10,000 IU, 5000IU and 2500 IU, respectively. The ongoing pregnancy rates per PCOS patient receiving hCG were 26.9% (7 of 26),30.8% (8 of 26) and 34.8% (8 of 23), respectively • A decrease in the dose of hCG used to trigger final oocyte maturation does not appear to affectadversely the probability of pregnancy in PCOS patients treated by IVF using GnRH antagonists and recombinantFSH Efstratios M. Kolibianakis, 2007
Ganirelix acetate causes a rapid reduction in estradiol levels without adversely affecting oocyte maturation in womenpretreated with leuprolide acetate who are at risk of ovarian hyperstimulation syndrome • 87 patients treated with long luteal (LL) or microdose flare (MDF) with ovarian hyperresponse and 87control patients without ovarian hyperresponse. • Inthe treatment group, there was a significant, reproducible reduction in serum E2 levels. Mean E2 at the start ofganirelix treatment was 4219.8 pg/ml and decreased in 24 h to 2613.7 pg/ml (36.7%; P < 0.001). An average of 24.9 ± 8.8oocytes were obtained at retrieval and an average of 19.1 ± 8.0 were metaphase II (79.2%). Fertilization occurred in13.9 ± 8.1 embryos (72.8%). In this high risk group, two cases of severe OHSS (2.3%) occurred. The ongoing pregnancyrate was 51.8%. Compared with the control group, there were no statistically significant differences in the rateof oocyte recovery, oocyte maturity, 2PN rate, fertilization, cancellation, OHSS or pregnancy. • GnRH-antagonist treatment of women pretreated with GnRH agonist rapidly reduced circulating serum E2 withoutadversely affecting oocyte maturation, fertilization rates or embryo quality and resulted in a high pregnancy rate inthis subgroup of patients at risk of OHSS. Robert L.Gustofson, 2006
Ovarian stimulation by concomitant administrationof cetrorelix acetate and HMG following Diane-35pre-treatment for patients with polycystic ovarysyndrome: a prospective randomized study pretreated with three cycles of Diane-35, followed by 0.25mg of cetrorelix on cycle day 3. From day 4, cetrorelix and gonadotrophin were administered concomitantly until the day of HCG injection Jiann-Loung Hwang, 2004
Premature luteinization Serum Progesterone elevation (> 1.0-1.5 ng/mL) at the end of the follicular phase, before hCG administration *5-35 % of cycles with a GnRH agonist (Edelstein et al, 1990, Silverberg et al, 1991) *20-38% of cycles with a GnRH antagonist ( Ubaldi et al, 1996. Bosch et al, 2003)
Premature luteinization and in vitro fertilizationoutcome in gonadotropin/gonadotropin-releasinghormone antagonist cycles in women with polycysticovary syndrome Shimon Segal, 2008
Gonadotropin-releasing hormone antagonist and metformin fortreatment of polycystic ovary syndrome patients undergoing in vitrofertilization–embryo transfer M M NICOLA DOLDI, 2006
Initiation of GnRH antagonist on Day 1 of stimulation ascompared to the long agonist protocol in PCOS patients.A randomized controlled trial: effect on hormonal levelsand follicular development Trifon G.Lainas, 2007
Theprimary outcome was E2 level on Day 5 of stimulation, while secondary outcomes were follicular development, LHduring ovarian stimulation and progesterone levels • Significantly more follicles on days 5, 7 and 8 of stimulation,significantly higher estradiol (E2) levels on days 1, 3, 5, 7 and 8 and significantly higher progesterone levels ondays 1, 5 and 8 of stimulation were observed in the antagonist when compared with the agonist group. • E2 was approximatelytwice as high in the antagonist when compared with the agonist group on day 5 of stimulation (432 versus • 204 pg ml21, P < 0.001). These differences were accompanied by significantly lower LH levels on days 3 and 5 and significantly • higher LH levels on days 1, 7 and 8 of stimulation in the antagonist when compared with the agonist group.
Clinical outcome from comparative studies on gonadotrophin-releasing hormone antagonist (GnRH-ant) versusgonadotrophin-releasing hormone agonist (GnRHa) protocol in PCOS patients Georg Griesinger, 2006
GnRH agonist for triggering final oocyte maturation in theGnRH antagonist ovarian hyperstimulation protocol: asystematic review and meta-analysis P<0.03 favors hCG P:0.05 favors lower risk after hCG G.Griesinger, 2005
GnRH agonist for triggering final oocyte maturationin patients at risk of ovarian hyperstimulationsyndrome: still a controversy S. Kol, 2008
Triggering with human chorionic gonadotropin ora gonadotropin-releasing hormone agonist ingonadotropin-releasing hormone antagonist-treatedoocyte donor cycles: findings of a large retrospectivecohort study • A total of 1171 egg donors performing 2077 stimulation cycles. • The proportion of mature oocytes was comparable, whereas the difference in the fertilization ratereached statistical significance (65% vs. 69%). No significant differences were observed in the implantationrate or clinical and ongoing pregnancy rates per ET. • The incidence of moderate/severe OHSS was 1.26% (13/1031; 95% confidence interval [CI], 0.74–2.15) and 0% (0/1046; 95% CI, 0.00–0.37) in the rhCG and GnRHagonist groups, respectively • Recipient outcome was not significantly different when using oocytes from GnRH antagonist–treated donor cycles triggered with hCG or GnRH agonist. However, GnRH agonist triggering was associatedwith a lower incidence of moderate/severe OHSS in egg donors Daniel Bodri, 2008
GnRH agonist to induce oocyte maturationduring IVF in patients at high risk of OHSS GnRHa + GnRH antagonis vs. OCP+ GnRHa+hCG Lawrence Engmann, 2006
The use of gonadotropin-releasing hormone (GnRH)agonist to induce oocyte maturation after cotreatmentwith GnRH antagonist in high-risk patients undergoingin vitro fertilization prevents the risk of ovarianhyperstimulation syndrome: a prospective randomizedcontrolled study • Sixty-six patients under 40 years of age with polycystic ovarian syndrome, polycystic ovarian morphology,or previous high response undergoing IVF Patients were randomized to an ovarian stimulation protocol consisting of either GnRH agonist trigger after cotreatment with GnRH antagonist (study group) or hCG trigger after dual pituitary suppression with a GnRH agonist (control group). • None of the patients in the study group developed any form of OHSS compared with 31% (10/32) of the patients in the control group. There were no significant differences in the implantation(22/61 [36.0%] vs. 20/64 [31.0%]), clinical pregnancy (17/30 [56.7%] vs. 15/29 [51.7%]), and ongoing pregnancy rates (16/30 [53.3%] vs. 14/29 [48.3%]) between the study and control groups, respectively. • The use of a protocol consisting of GnRH agonist trigger after GnRH antagonist cotreatment • combined with adequate luteal phase and early pregnancy E2 and P supplementation reduces the risk of OHSS in high-risk patients undergoing IVF without affecting implantation rate Lawrence Engmann, 2008