Download
1 / 6
60 likes | 224 Views
Weekly HSE Lateral Learning 13/06/05. Slide 1/3. 31/05/05 NDSC Fatality B4P B4P

E N D
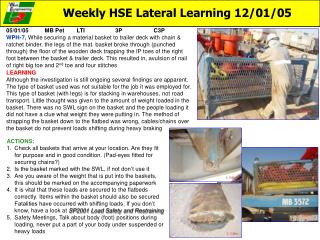
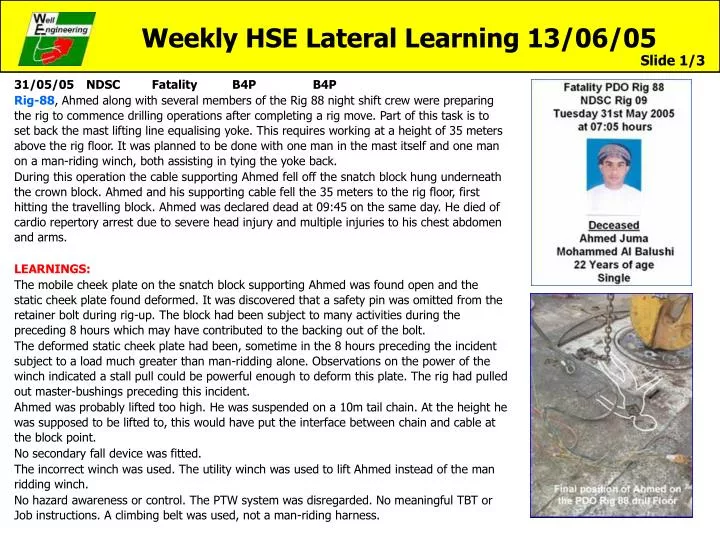
Weekly HSE Lateral Learning 13/06/05 Slide 1/3 31/05/05 NDSC Fatality B4P B4P Rig-88, Ahmed along with several members of the Rig 88 night shift crew were preparing the rig to commence drilling operations after completing a rig move. Part of this task is to set back the mast lifting line equalising yoke. This requires working at a height of 35 meters above the rig floor. It was planned to be done with one man in the mast itself and one man on a man-riding winch, both assisting in tying the yoke back. During this operation the cable supporting Ahmed fell off the snatch block hung underneath the crown block. Ahmed and his supporting cable fell the 35 meters to the rig floor, first hitting the travelling block. Ahmed was declared dead at 09:45 on the same day. He died of cardio repertory arrest due to severe head injury and multiple injuries to his chest abdomen and arms. LEARNINGS: The mobile cheek plate on the snatch block supporting Ahmed was found open and the static cheek plate found deformed. It was discovered that a safety pin was omitted from the retainer bolt during rig-up. The block had been subject to many activities during the preceding 8 hours which may have contributed to the backing out of the bolt. The deformed static cheek plate had been, sometime in the 8 hours preceding the incident subject to a load much greater than man-ridding alone. Observations on the power of the winch indicated a stall pull could be powerful enough to deform this plate. The rig had pulled out master-bushings preceding this incident. Ahmed was probably lifted too high. He was suspended on a 10m tail chain. At the height he was supposed to be lifted to, this would have put the interface between chain and cable at the block point. No secondary fall device was fitted. The incorrect winch was used. The utility winch was used to lift Ahmed instead of the man ridding winch. No hazard awareness or control. The PTW system was disregarded. No meaningful TBT or Job instructions. A climbing belt was used, not a man-riding harness.
Weekly HSE Lateral Learning 13/06/05 Slide 2/3 • Aimed at PDO DSV’s: Some simple checks on your rig to prevent a similar occurrence • Check what kind of man-riding procedures are in place on your unit, review them and highlight violations. To which height is man-riding allowed, are there any jobs that will require breaking this height rule? • Are all man-riding activities controlled with a PTW. Have a look back at the PTW record does it match with the activities undertaken • Is there a secondary fall device installed below the sheave. In its simplest form this is a wire sling suspended independently such that if there is a catastrophic failure of the sheave the wire will be caught • Are man riding belts in use and what type, the photo show a climbing belts not a man riding belt, familiarise yourself with what constitutes a man riding belt • Is there a dedicated Man riding winch, does it meet the requirements for a man riding winch, check with contractor, is it used for any other purpose. What is the pulling power of this winch? Use the manufactures stall load, unless you know the actual pull • What types of shackles are used to connect the snatch blocks to the respective pad eyes. • Do they have a dedicated number and are they part of the Lifting equipment register • Conduct a mast inspection together with the Rig Manager and assure your self that: • all sheaves/snatch blocks are properly secured • right type of shackles are in use ( see attached 2003 HSE info note next slide) • all shackles are secured with the right safety pin (no welding wire). • Check your findings against the latest Mast inspection check list of your unit and investigate major deficiencies. • Before such activities that ensure that hazard awareness controls are in place e.g. a JSA, check quality TBT’s are carried out • Use the Rig HSE File This is a climbing belt not a man riding belt
Weekly HSE Lateral Learning 13/06/05 Slide 3/3 Simple Guide to Shackle Use 4 types of shackle available 2/ Round Pin Bow Shackle 1/ Screw Pin Bow Shackle • Single Lifts, no vibration or significant movement • 2. Permanent fixture, not regularly opened and closed • 3. For used with chains • 4. For use on moving items (and vibration) or items out of sight 3/ Screw Pin “D” Shackle 4/ Safety Type Bow Shackle Type 4 shackle will be used for suspending sheaves in mast
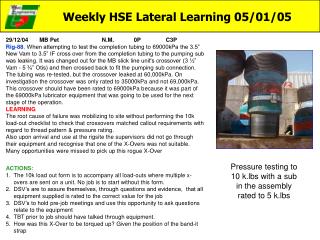
Weekly HSE Lateral Learning 18/05/05 20/02/05 Dalma NM 1A B3P Rig 53 While pressurising to set 9 5/8” whipstock the mud pump pressure increased to 12000 kpa and stopped. The pump stroke gauge read zero. The supervisors suspected that the pump had tripped. The Chief Electrician checked and reported everything was OK. While this check was ongoing TP opened up test pump to apply final test pressure, the test pump Pressure gauge indicated 29000 kpa! LEARNING In fact 29000 kPa had been applied to system by the mud pumps, the pumps had stalled due to pressure and the pop off valve had failed. Investigations observed that the stand pipe manifold pressure gauge hose had ruptured causing the sensor diaphragm to fail.. The gauge of remote choke panel was also connected to same sensor. (MULTIPLE GAUGES ON ONE SENSOR) The relief valves did not function even at 29000 kPa. Mud pumps relief valves were set & tested to 19000 kPa on 31.1.05, The relief valves were found stuck as dried out mud was found to have hardened on top of piston, mud was allowed to accumulate against the valve because of the backward slope of the pipe Picture 2 ACTIONS 1. Check on your rig: the piping arrangement from the pressure relief valves to the tank, this piping needs to be - Sloping downward to prevent mud settling and drying against the valve - Be straight, no bends - Be anchored securely at the tank end - Be made of piping rated equal to the system pipework 2. All gauges must have a separate sensor, with the exception of monitoring devices such as geolographs 3. Have pressure gauges (analog type) installed on standpipe manifold, visible for the driller and crew
Weekly HSE Lateral Learning 29/04/05 15/04/05 OD&E LTI 3P C4P RIG-40,During a routine interwell rig move, the rig carrier sustained a flat tyre. The rig carrier was raised off the ground and the surrounding sandy area was leveled. The bolts holding the wheel retaining wedges where loosened and some of the retaining wedges were removed. The plan was to move the forklift into position to support the wheel prior to removing the last of the retaining wedges. As the wheel was slowly turned by hand, it came off the hub and fell over. The Junior Mechanic and Derrickman tried to jump clear but their legs were hit by the falling wheel. The Derrickman sustained a broken leg. The Junior Mechanic had bruising to his wrist and leg. LEARNING The job appeared to have been reasonably well planned and supervised. A ToolBox Talk was held, although the operational aspects were well covered safety aspects were not, no procedures were in place, the area was prepared and the right tools were being used. Previous experience of all involved was that these wheels are tight on their hubs and require a lot of effort to remove, this time it fell off unexpectedly Always Expect the Unexpected…and Plan for it. • ACTIONS • A quality TBT/JSA prior to such a job is vital. Ask the “what if’s”What if the wheel falls, what escape route does the team haveWhat is different now, is the wheel hot? • It is apparent now that this very hazardous job, no procedures were in place or JSA done. This is a 2.8 ton wheel, the removal of which requires men to stand in front of it while loosening its retaining bolts. Work such as this needs in depth planning, but firstly the rigsite teams need to be able to recognize what constitutes a hazardous job. It is the responsibility of the senior personal on site to be able to recognize such hazards, and protect their workers • Although the medivac went well, The Thuraiya belonging to the DSV failed to operate during this emergency. All rigs to check their emergency contact systems weekly, you never know when you need them The Senior Mechanic, standing directly in front of the wheel and turning it. when the wheel fell off he was able to duck through the center hole. he was very fortunate to escape unharmed. The wheel passed over him!
Weekly HSE Lateral Learning 06/04/05 30/03/05 Schlum (Reda) PDO 2P C3P WPH-15,While preparing to connect lifting chains to ESP motor clamp, the motor rolled slightly and pinched the technician’s left index finger at the 3rd digit. Although employee was wearing proper PPE gloves, the pinch resulted in a cut approximately ½ inch in length and required 6 stitches LEARNING The technician was working alone, attempting to move a heavy load sufficiently to secure a lifting device. This was made all the more difficult by the grove in the catwalk. The grove had trapped the ESP pump, the lifting lugs made it difficult to turn. Thought should have gone into how this pump was going to be handled on a catwalk with a large grove in the middle, rollers are used at the other end Was a Toolbox talk held for this job was it effective? Is their procedures for handling pumps? • ACTIONS: • Do you have a similar catwalk with large grove, what additional problems does this cause you? how do you manage this hazard? It needs thought about before you start to place large heavy objects on it, not after you’ve hurt someone • The step by step approach to handing a large item such as an ESP pump should have been detailed in the toolbox talk, • Ask for assistance, when manoeuvring difficult objects first look at mechanical means, if this is not possible do it as a coordinated team