Download
1 / 24
240 likes | 256 Views
B LOOD PRESS UR E. un its u s e d in m ed ici ne : m m H g = 0 . 13 3 kP a , kP a = 7 . 5 mm H g. B lo o d ve ss e ls c on t a in b lo o d t ha t e x er t s o n t he ir w a lls a pre ss ur e. 1 ) A rteri a l a nd v e n o us p re ss ur e s dep e nd on. vascular volume blood volume

E N D
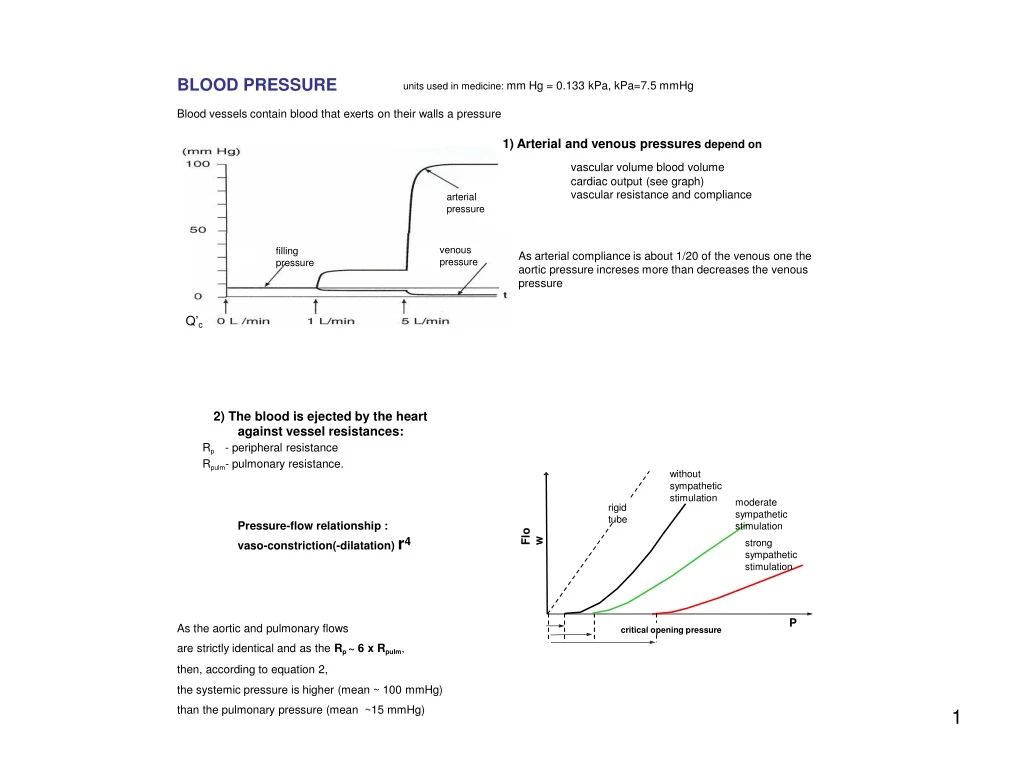
BLOODPRESSURE unitsusedinmedicine:mm Hg=0.133 kPa,kPa=7.5mmHg Bloodvesselscontain bloodthat exertson their walls apressure 1)Arterial andvenous pressuresdependon vascular volume blood volume cardiac output (see graph) vascular resistance and compliance arterial pressure venous pressure filling pressure Asarterial complianceis about 1/20ofthe venousone theaortic pressureincresesmore thandecreasesthevenous pressure Q’c 2) The blood is ejected by the heart against vessel resistances: Rp - peripheral resistance Rpulm- pulmonary resistance. without sympathetic stimulation moderate sympathetic stimulation rigid tube Pressure-flow relationship : vaso-constriction(-dilatation) r4 Flow strong sympathetic stimulation P As the aortic and pulmonary flows are strictly identical and as the Rp ~ 6 x Rpulm, then, according to equation 2, the systemic pressure is higher (mean ~ 100 mmHg) than the pulmonary pressure (mean ~15 mmHg) criticalopening pressure
BLOODPRESSURE unitsusedinmedicine:mm Hg=0.133 kPa,kPa=7.5mmHg Bloodvesselscontain bloodthat exertson their walls apressure 1)Arterial andvenous pressuresdependon vascular volume blood volume cardiac output (see graph) vascular resistance and compliance arterial pressure venous pressure filling pressure Asarterial complianceis about 1/20ofthe venousone theaortic pressureincresesmore thandecreasesthevenous pressure Q’c 2) The blood is ejected by the heart against vessel resistances: Rp - peripheral resistance Rpulm- pulmonary resistance. without sympathetic stimulation moderate sympathetic stimulation rigid tube Pressure-flow relationship : vaso-constriction(-dilatation) r4 Flow strong sympathetic stimulation P As the aortic and pulmonary flows are strictly identical and as the Rp ~ 6 x Rpulm, then, according to equation 2, the systemic pressure is higher (mean ~ 100 mmHg) than the pulmonary pressure (mean ~15 mmHg) criticalopening pressure
3) Arterial PULSE As Q’c is intermittent, the arterial pressure oscillates between - a maximum (systolic pressure: Ps) - a minimum (diastolic pressure: Pd): Ps aorta femoralartery dicrotic wave 100mmHg Pmean 95mmHg Pd Ps- Pd= pulseP aorta branching 4)Measurementofbloodpressure: direct - catheterisation indirect - sphygmomanometry: mercury manometer connected to brachial manchette stethoscope (auscultation of brachial pulse) a) brachial atery is compressed by manchette inflating b) slow deflating until 1st sounds audible: Psyst c) slow deflating until the last sound: Pdiast noflow turbulent flow:beats laminarflow sound intensity Normalvalues: Hypertension: Ps > 140 and/or Pd > 90
3) Arterial PULSE As Q’c is intermittent, the arterial pressure oscillates between - a maximum (systolic pressure: Ps) - a minimum (diastolic pressure: Pd): Ps aorta femoralartery dicrotic wave 100mmHg Pmean 95mmHg Pd Ps- Pd= pulseP aorta branching 4)Measurementofbloodpressure: direct - catheterisation indirect - sphygmomanometry: mercury manometer connected to brachial manchette stethoscope (auscultation of brachial pulse) a) brachial atery is compressed by manchette inflating b) slow deflating until 1st sounds audible: Psyst c) slow deflating until the last sound: Pdiast noflow turbulent flow:beats laminarflow sound intensity Normalvalues: Hypertension: Ps > 140 and/or Pd > 90
06.10.2014 PERIPHERALRESISTANCE (units:N.s/m5ormmHg.s/mlblood) =resistancethatthe vasculartree(arteriolesinparticular)opposestobloodflow. Remember: One should discuss the impedance rather than resistance. However, on 1st approximation, the Hagen-Poiseuille equation is used: 2factors:geometry viscosity R1 R2 R3 R4 R1 R R3 2 Rtot=R1+R2+R3+...Rn because 22 a) geometry: l - the length of vessels increases with growth and remains constant in adults - thelengthof systemicvesselsis greater thanthatof pulmonaryvessels(henceRp>Rpulm) r4- smallshortening(relaxation)ofvascularmusclecells->greatvariationsofflux S1v1=S2v2 =>v1>v2=> Ekin1>Ekin2 - r irregular: case of aneurysma P1 T2 P2 Then (energy conservation): P2 > P1 and T2 > T1 Result: - slow flow (thrombosis) - wall thinning (rupture: bleeding!) T1 caseofstenosis IfR*>2000: laminarflow→turbulent flow: murmur 23 *Reynoldsnumber:2r.v.r/h 13
06.10.2014 PERIPHERALRESISTANCE (units:N.s/m5ormmHg.s/mlblood) =resistancethatthe vasculartree(arteriolesinparticular)opposestobloodflow. Remember: One should discuss the impedance rather than resistance. However, on 1st approximation, the Hagen-Poiseuille equation is used: 2factors:geometry viscosity R1 R2 R3 R4 R1 R R3 2 Rtot=R1+R2+R3+...Rn because 22 a) geometry: l - the length of vessels increases with growth and remains constant in adults - thelengthof systemicvesselsis greater thanthatof pulmonaryvessels(henceRp>Rpulm) r4- smallshortening(relaxation)ofvascularmusclecells->greatvariationsofflux S1v1=S2v2 =>v1>v2=> Ekin1>Ekin2 - r irregular: case of aneurysma P1 T2 P2 Then (energy conservation): P2 > P1 and T2 > T1 Result: - slow flow (thrombosis) - wall thinning (rupture: bleeding!) T1 caseofstenosis IfR*>2000: laminarflow→turbulent flow: murmur 23 *Reynoldsnumber:2r.v.r/h 13
06.10.2014 Vasculartree: R. atrium R. ventricle Pulm. Art. Capillaries Pulm.veins L. atrium L. ventricle Aorta Arterioles Capillaries Arteries Veines Arterial ramification: ↑ of total section ↓ of blood velocity Bloodvolume fraction A weak DP is sufficient to maintain the capillary perfusion, because: Rtot < Rindiv. remember Bloodpressure (mmHg) Rtot 1 2 -1=R-1+R-1+ ... R -1 i Totalsection(m2) Thefall of meanarterial pressureis relativelyweak alongthearteries but Bloodvelocity(cm/s) becomessteepat the levelofarterioles: arteriolesdeterminethe peripheralresistance 24 25 14
06.10.2014 Vasculartree: R. atrium R. ventricle Pulm. Art. Capillaries Pulm.veins L. atrium L. ventricle Aorta Arterioles Capillaries Arteries Veines Arterial ramification: ↑ of total section ↓ of blood velocity Bloodvolume fraction A weak DP is sufficient to maintain the capillary perfusion, because: Rtot < Rindiv. remember Bloodpressure (mmHg) Rtot 1 2 -1=R-1+R-1+ ... R -1 i Totalsection(m2) Thefall of meanarterial pressureis relativelyweak alongthearteries but Bloodvelocity(cm/s) becomessteepat the levelofarterioles: arteriolesdeterminethe peripheralresistance 24 25 14
06.10.2014 Capillarybed Ø 4-10mm; 0.1-3 mm blood speed: 0.5 mm/s capillaries lymphatic capillary vein arteriole arterio- venous metarteriole precapillary preferential channel venule anastomose sphincters 26 Capillaryexchanges smallthickness shortdistancetosurroundingcells facilitating capillary (endothelial) exchanges: slowbloodflow 1)diffusion 2)ultrafiltration 3)transcytosis 4)diapedesis 27 15
06.10.2014 Capillarybed Ø 4-10mm; 0.1-3 mm blood speed: 0.5 mm/s capillaries lymphatic capillary vein arteriole arterio- venous metarteriole precapillary preferential channel venule anastomose sphincters 26 Capillaryexchanges smallthickness shortdistancetosurroundingcells facilitating capillary (endothelial) exchanges: slowbloodflow 1)diffusion 2)ultrafiltration 3)transcytosis 4)diapedesis 27 15
06.10.2014 ULTRAFILTRATION: transport of fluid across the endothelium per unit time At a given place of a capillary, ultrafiltration is written as: Pi Pc pc pi transportoffluidacrossthecapillary . LpA=KF filtration coefficient hydraulicconductance(cm3/s/dyne) areaofexchange reflexioncoefficient(formacromolecules) capillaryandinterstitialhydrostaticpressures capillaryandinterstitialoncoticpressures Jv>0 :filtration Jv<0 :(re)absorption 28 Caseoftheskeletalmuscle Thevalue of Jvvaries along thecapillary andalsobetweenadjacentcapillaries. Thus, the fluid filtered at the arterial pole is taken up at the venous pole or by neighbouring capillaries. Thefluidthat escapedtoreabsorptionis takenupbythelymphaticcapillaries. 29 16
06.10.2014 ULTRAFILTRATION: transport of fluid across the endothelium per unit time At a given place of a capillary, ultrafiltration is written as: Pi Pc pc pi transportoffluidacrossthecapillary . LpA=KF filtration coefficient hydraulicconductance(cm3/s/dyne) areaofexchange reflexioncoefficient(formacromolecules) capillaryandinterstitialhydrostaticpressures capillaryandinterstitialoncoticpressures Jv>0 :filtration Jv<0 :(re)absorption 28 Caseoftheskeletalmuscle Thevalue of Jvvaries along thecapillary andalsobetweenadjacentcapillaries. Thus, the fluid filtered at the arterial pole is taken up at the venous pole or by neighbouring capillaries. Thefluidthat escapedtoreabsorptionis takenupbythelymphaticcapillaries. 29 16
06.10.2014 Modificationofultrafiltrationparameters: oedema - accumulation of fluid in the interstitial space - loss of fluid from the interstitial space dehydratation arteriolar vasodilatation (e.g., exposure to heat) haemoconcentration (e.g. transpiration) 30 subatmospheric pressure! VEINS are large and have very thin walls (great compliance -> veins are blood reservoirs) 60cm In standing position, the venous pressure becomes: subatmospheric in the head and neck (-mgh) high in abdomen and legs (+mgh): risk of oedema 110cm Gravitation:rgh 95–45= 50 -35= 10-45 100 95 95 2 100 10 10 2 95+ 80= 175 90= 10+ 80 31 17
06.10.2014 Modificationofultrafiltrationparameters: oedema - accumulation of fluid in the interstitial space - loss of fluid from the interstitial space dehydratation arteriolar vasodilatation (e.g., exposure to heat) haemoconcentration (e.g. transpiration) 30 subatmospheric pressure! VEINS are large and have very thin walls (great compliance -> veins are blood reservoirs) 60cm In standing position, the venous pressure becomes: subatmospheric in the head and neck (-mgh) high in abdomen and legs (+mgh): risk of oedema 110cm Gravitation:rgh 95–45= 50 -35= 10-45 100 95 95 2 100 10 10 2 95+ 80= 175 90= 10+ 80 31 17
06.10.2014 ( periph. venous P - central venous P ) venous Resistance ~5-10mmHg same as Q’c Venousreturn = verylow The veins are large and have very thin walls (great compliance -> veins are blood reservoirs) Due to the vascular convergence, the blood velocity increases, but the flow is less pulsatile. Intheextremities(butnot in theskullor inthorax), theveins havevalves The venous return is increased by: - laying down (shock: elevation of extremities) - venoconstriction (mobilisation of blood reserves) - deep inspirations - compression of veins by skeletal muscles recumbent standing walking sitting Pressureinthemalleolarvein(mmHg) 32 Distributionofcardiacoutput andofoxygenuptake Restingcondition: Activity: increase of cardiac output vasodilatation in active organs vasoconstriction in inactive organs lungs The capacity of vaso(constriction/dilatation) varies from one organ to another: left heart right heart of of coronary brain kidney brain heart liver bloodflow(l/min) skin muscles liver intestine kidney skin 33 18
06.10.2014 ( periph. venous P - central venous P ) venous Resistance ~5-10mmHg same as Q’c Venousreturn = verylow The veins are large and have very thin walls (great compliance -> veins are blood reservoirs) Due to the vascular convergence, the blood velocity increases, but the flow is less pulsatile. Intheextremities(butnot in theskullor inthorax), theveins havevalves The venous return is increased by: - laying down (shock: elevation of extremities) - venoconstriction (mobilisation of blood reserves) - deep inspirations - compression of veins by skeletal muscles recumbent standing walking sitting Pressureinthemalleolarvein(mmHg) 32 Distributionofcardiacoutput andofoxygenuptake Restingcondition: Activity: increase of cardiac output vasodilatation in active organs vasoconstriction in inactive organs lungs The capacity of vaso(constriction/dilatation) varies from one organ to another: left heart right heart of of coronary brain kidney brain heart liver bloodflow(l/min) skin muscles liver intestine kidney skin 33 18
06.10.2014 Principleofaregulatoryloop (example:controlof ventilation&cardiacoutput) descendentcontrol anticipation, effort, emotion, fear... dependentvariables receptors P E R T U R B A T I O N S carotid glomus brain stem PO2 PCO2 pH set points cover peripheral metabolic needs! arterial pressure carotidsinus CNS &ANS controlledvariables effectors VENTILATION muscles, lung, heart, vessels, controlcenters CARDIACOUTPUT intrinsic&local factors action potentials = setpoints= ongoingactivity in specialisedneuronalcircuits 34 Regulationofbloodpressure high arterialpressure normal low nervefromcarot.sinus vagusnerveto heart frequency + - + contractility - sympatheticnervestoheart vasotonus + - surrenal gland: adrenaline sympatheticnervestovessels 35 19
06.10.2014 Principleofaregulatoryloop (example:controlof ventilation&cardiacoutput) descendentcontrol anticipation, effort, emotion, fear... dependentvariables receptors P E R T U R B A T I O N S carotid glomus brain stem PO2 PCO2 pH set points cover peripheral metabolic needs! arterial pressure carotidsinus CNS &ANS controlledvariables effectors VENTILATION muscles, lung, heart, vessels, controlcenters CARDIACOUTPUT intrinsic&local factors action potentials = setpoints= ongoingactivity in specialisedneuronalcircuits 34 Regulationofbloodpressure high arterialpressure normal low nervefromcarot.sinus vagusnerveto heart frequency + - + contractility - sympatheticnervestoheart vasotonus + - surrenal gland: adrenaline sympatheticnervestovessels 35 19
06.10.2014 Adaptation to exercise During physical effort, the increased metabolic demand of muscle cells must be covered by Increased flows of substrates (glucose, fatty acids, O2) and products (CO2, lactate). In case of strenuous exercise, the blood flow to heart increases 4x, to skeletal muscle 20x, does not change to brain and decreases to other tissues. a) short term adaptation: ↑ of cardiac output ↑ of blood flow to muscles ↑ of ventilation ↑ of O2 extraction ↑ of thermal dissipation H+ neutralisation substrate mobilisation (liver, adipose tissue) arterialblood arterio-venousdifference ↓ Power(W) O2uptakeL/min 36 O uptakeL/min 2 Artificial pacemakers • Implantable devices with 2 principal components: - generator of impulsions, containing abattery (Lithium) and electronic circuits (oscillators, microprocessor, memory…) - electrodes used to stimulate the cardiac muscle and to record its activity • Thestimulatorbodyis generallyimplantedwithinthe subclavian subcutaneous adipous tissue The electrode leads are introduced into the cardiac cavities • by catheterisation through the sublavian and superior cava veins. They are anchored in the walls of the right atrium point). (signalsfromthesinusnode)andventricle(stimulation • Biocompatibility:titaniumenvelope(biologicallyinert) • Programmability: numerous parameters may be modified after the implantation, namely, systolic frequency and stimulation threshold • Telemetry: programmation/interrogation of the pacemaker from the exterior • Servo-control: automatic adaptation of the stimulating requency with respect to metabolic needs of thee patient, e.g., ventricle stimulation frequency follows sinusal discharge 37 20
06.10.2014 Adaptation to exercise During physical effort, the increased metabolic demand of muscle cells must be covered by Increased flows of substrates (glucose, fatty acids, O2) and products (CO2, lactate). In case of strenuous exercise, the blood flow to heart increases 4x, to skeletal muscle 20x, does not change to brain and decreases to other tissues. a) short term adaptation: ↑ of cardiac output ↑ of blood flow to muscles ↑ of ventilation ↑ of O2 extraction ↑ of thermal dissipation H+ neutralisation substrate mobilisation (liver, adipose tissue) arterialblood arterio-venousdifference ↓ Power(W) O2uptakeL/min 36 O uptakeL/min 2 Artificial pacemakers • Implantable devices with 2 principal components: - generator of impulsions, containing abattery (Lithium) and electronic circuits (oscillators, microprocessor, memory…) - electrodes used to stimulate the cardiac muscle and to record its activity • Thestimulatorbodyis generallyimplantedwithinthe subclavian subcutaneous adipous tissue The electrode leads are introduced into the cardiac cavities • by catheterisation through the sublavian and superior cava veins. They are anchored in the walls of the right atrium point). (signalsfromthesinusnode)andventricle(stimulation • Biocompatibility:titaniumenvelope(biologicallyinert) • Programmability: numerous parameters may be modified after the implantation, namely, systolic frequency and stimulation threshold • Telemetry: programmation/interrogation of the pacemaker from the exterior • Servo-control: automatic adaptation of the stimulating requency with respect to metabolic needs of thee patient, e.g., ventricle stimulation frequency follows sinusal discharge 37 20
06.10.2014 Recanalisation of coronary arteries 1 ANGIOPLASTY DILATATION STENT 2 BYPASS (anastomosis with mammary artery) 38 Artificialvalves Deployment of self expanding stent valve out of the tip of the catheter in sequential steps: After contact with blood the nitinol stent reaches its transformation temperature leading to an expansion of the proximal segment that carried the valve. After optimal positioning the distal part of the stent is released out of the catheter stabilising and anchoring the stent in the ascending aorta. Aorticvalvebased oncombination ofZstentandbovinejugularvein 39 21
06.10.2014 Recanalisation of coronary arteries 1 ANGIOPLASTY DILATATION STENT 2 BYPASS (anastomosis with mammary artery) 38 Artificialvalves Deployment of self expanding stent valve out of the tip of the catheter in sequential steps: After contact with blood the nitinol stent reaches its transformation temperature leading to an expansion of the proximal segment that carried the valve. After optimal positioning the distal part of the stent is released out of the catheter stabilising and anchoring the stent in the ascending aorta. Aorticvalvebased oncombination ofZstentandbovinejugularvein 39 21
R ECG rest: 0.8 - 0.9 s P T Cardiac cycle Q S (left heart) mmHg P systolic 120 di crotic wave L. ventricl e PRESSURE P diastolic 80 ventricular, aorta aortic, atrial a 40 L. atrium. v c 0 S YS DIASTOLE SYSTOLE Phases: 1 2a 2b 3 4a 4b 4c ml telediastolic v. 1 isovolumic contraction 12 Systolic volume 2 ejection 0 = ejected 3 isovolumic relaxation 80 VOLUME 4 filling telesystolic v. L. ventricle 40 0 Sound: I II III III IV PCG Mitral valve O O F F ECHO F O O N.B. Aortic valve Pressure in ml / s the right ventricle: 800 FLOW 20 - 30/0 - 5 mm Hg aorta 400 0
R ECG rest: 0.8 - 0.9 s P S e c T di crotic wave v a Cardiac cycle Q (leftheart) mmHg 120 P systolic L. ventricl PRESSURE ventricular, aortic, atrial P diastolic 80 aorta 40 L. atrium. 0 S YS DIASTOLE SYSTOLE 1 I 2a O 2b 3 F 4a II 4b 4c III O F ml 120 telediastolic v. Systolic volume = ejected 80 VOLUME L. ventricle telesystolic v. 40 0 Sound: III IV PCG Mitral valve Phases: 1 isovolumic contraction 2 ejection 3 isovolumic relaxation 4 filling F O ECHO O N.B. Pressure in the right ventricle: 20-30/0-5 mm Hg Aortic valve ml / s 800 FLOW aorta 400 0