Download
1 / 63
640 likes | 690 Views
Learn about the differences between somatic and autonomic nervous systems, the efferent neurons, and the Sympathetic and Parasympathetic divisions. Explore Cholinergic and Adrenergic nervous fibers, neurotransmitters, and receptor types.

E N D
Autonomic nervous systemCholinergic agonists (CHOLINOMIMETICS) PhD. A.V. Aleksandrova
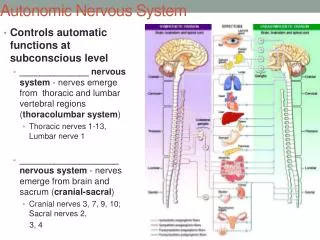
Somatic N.SAutonomic N.S Control skeletal muscles Control internal viscera Voluntary Involuntary Somatic nerve is one autonomic nerve is fiber two fibers(Preganglionic &Postganglionic) What are the differences between the somatic and the autonomic nervous system?
Sympathetic ANS • The 1st neuron of sympathetic division is located in the thoracolumbar region of the spinal cord (T1-L3) and the 2nd is disposed either in the paravertebral, or in the prevertebral ganglia. Postganglionic non-myelinated nerve fibres arising from neurones in the ganglia, innervate most organs of the body • The neurotransmitter released by sympathetic nerve endings is noradrenaline.
Parasympathetic system • The 1st neuron of parasympathetic system is located in the brain stem and in the sacral region of the spinal cord. The preganglionic fibres leave the central nervous system in the III, VII, IX and X pairs of cranial nerves and the third and fourth sacral spinal roots. • Ganglia are located either in the tissue of effector organ or near it. The nerve endings of the postganglionic parasympathetic fibres release neurotransmitter acetylcholine. All the preganglionic nerve fibres (sympathetic and parasympathetic;) are myelinated and release acetylcholine from the nerve terminals which depolarizes the ganglionic neurones by activating nicotinic receptors.
Cholinergic nervous fibres are: 1) preganglionic (sympathetic and parasympathetic); 2) all postganglionic parasympathetic; 3) postganglionic sympathetic which supply sweat glands and vessels of skeletal muscles; 4) somatic nerves; 5) nerves which supply adrenal medulla and carotic sinuses; 6) neurons of CNS Adrenergicnervous fibres are: 1) postganglionic sympathetic, except those which supply sweat glands and vessels of skeletal muscles; 2) neurons of CNS
Cholinergic transmission Main NT is Acetylcholine (Ach). A large number of peripheral ANS fibers which synthesize & release Acetylcholine are called CHOLINERGIC fibers. They include: • All pre-ganglionic efferent autonomic fibers. • Somatic motor fibers to skeletal muscles. • Most parasympathetic post ganglionic fibers. • A few sympathetic post ganglionic fibers– to sweat glands. Some parasympathetic post ganglionic fibers utilize nitric oxide or peptides for transmission.
Fate of acetylcholine released by cholinergic fiber • ACh is released from the nerve into the synaptic cleft and binds to ACh receptors on the post-synaptic membrane, relaying the signal from the nerve. • Ach-esterase, located on the post-synaptic membrane, terminates the signal transmission by hydrolyzing ACh. • The liberated choline is reuptaken by the pre-synaptic membrane and used for resynthesis of ACh.
Cholinergic synapse • Nerve terminal of cholinergic fibre contains numerous vesicles with neurotransmitter acetylcholine (ACh) that is released from presynaptic membrane. • Release of acetylcholine depends on sufficient influx of Ca 2+, which occurs under the influence of action potential. ATP negative feedback ATP
Cholinergic receptor types • Two cholinergic receptor subtypes have been identified by selective agonists: muscarinic (M-cholinoceptors) and nicotinic (N-cholinoceptors). At least 5 subtypes of muscarinic receptors (M1 – M5) have been distinguished. • There are 3 main classes of N- cholinoceptors: the muscle, ganglionic, and CNS classes. MUSCARINIC NICOTINIC M1 NM M5 NN M2 M4 M3 • Ganglions • Carotid sinus • Skeletal muscles • Adrenal glands • CNS • Eye • Heart • Smooth muscles • Exocrine glands • CNS
Muscarinic receptors • High affinity to muscarine • M1 – gastric parietal cells, saliva, CNS • M2 - cardiac cells, smooth muscle, CNS • M3 - bladder, exocrine glands, smooth muscle, eye, CNS • M1&M3 – Gq • M2 - Gi Amanita muscaria
Nicotinic receptors • High affinity to nicotine • NM- neuro-muscular junction • NN – ganglion, adrenal gland CNS, carotid sinus
Mechanisms of impulse transmission • Muscarinic receptors belong to G-protein coupled receptors. Transmission of impulses throughM1, M3, M5 cholinoceptors is realized by phospholipase C, inositol triphosphate and diacylglycerol • Stimulation of M2 and M4 cholinoceptors results in inhibition of adenylate cyclase and decrease in intracellular cAMP. • N- cholinoceptors are ion channel coupled. Their stimulation results in opening of Na+ channels that causes depolarization.
Muscarinic receptors M1 M3
Nicotinic actions Skeletal muscles: • Low conc. of nicotine muscle contraction • High conc. of nicotine persistent depolarization & relaxation. Ganglia: stimulation of sympathetic& parasympathetic ganglia. Adrenal medulla release of catecholamines (A & NA).
I. Direct acting 1. Muscarinic agonists (M-cholinomimetics) Pilocarpine Oxothermorine Aceclidine 2. Nicotinic agonists Lobeline Dimethylphenylpiperazinum (DMPP) 3. Muscarinic and nicotinic agonists Acethylcholine Carbachol II. Indirect acting (muscarinic and nicotinic agonists – anticholinesterase agents) 1. Reversible Neostigmine (Proserinum) Physostigmine Pyridostigmine Edrophonium Ambenonium chloride (Oxazylum) Galanthamine 2. Irreversible (Organophosphates) Echotiophate Isoflurophate Arminum Drugs used in poisoning with organophosphates 1. Reactivators of acetylcholine esterase Pralidoxime Dipiridoxinum Izonitrozinum Obidoxime 2. M-cholinoblockers Atropine Cholinomimetics
Pharmacological effects • Bradycardia, decrease in blood pressure • Raising the tone of smooth muscles of internal organs • Stimulation of intestinal motility • Reducing sphincter of alimentary canal and bladder • Increased secretory activity of the exocrine glands • Constriction of the pupil of the eye (miosis) • spasm of accommodation • Reducing intra ocular pressure • Relief of pulses in mionevralnomu skeletal muscle synapse, strengthening their contractility (anticholinergic drugs) • Stimulation of the central nervous system (means of penetrating the blood-brain barrier)
Main clinical usage • 1. Glaucoma (Pilocarpine, Physostigmine, Armine) • 2.Infants (Neostigmine) • 3.Postoperative atony of the intestines and bladder (Neostigmine) • 4. Paralysis, paresis, neuritis, polyneuritis (Neostigmine) • 5.Dusturbances of skeletal muscle contractile function after cranial trauma, polio and stroke (Galanthamine hydrobromide) • 6.Belladonna poisoning (Neostigmine, Physostigmine, Galanthamine) • 7. Overdose nondepolarizing muscle relaxants (Neostigmine) • 8. Xerostomia (Pilocarpine) • 9. Respiratory depression (Cititon, Lobeline)
Side effects of cholinomimetics • 1. Bradycardia • 2. Bronchospasm • 3. Intestinal cramps, colic, diarrhea • 4. Hypersalivation • 5. Blurred vision
Contraindications • 1. Bradycardia, A-V block • 2. Asthma • 3.Gastric ulcer and 12 duodenal ulcer • 4. Epilepsy (Neostigmine) • 5.Pregnancy (Neostigmine)
Direct acting cholinergic agonists ACETYLCHOLINE
Direct acting cholinergic agonists ACETYLCHOLINE • Decrease in heart rate and cardiac output 2. Decrease in blood pressure
Direct acting cholinergic agonists ACETYLCHOLINE 3. Other actions 4. Clinical use very rare: eye drops to obtain miosis • Muscarinic and nicotinic agonistnot used clinically because Ach is not selective (N, M) • Has short duration of action. Why? • Due to rapid metabolism by acetycholinesterase
Direct acting cholinergic agonists • Stimulation of atonic bladder • Nonobstructive urinary retention • Neurogenic atony • Megacolon Ophthalmology
Direct acting cholinergic agonists PILOCARPINE • Tertiary nitrogen • Good adsorbtion • Penetrate BBB
Direct acting cholinergic agonists PILOCARPINE Natural alkaloids Tertiary amine lipophilic Pharmacokinetics It is well absorbed Good distribution Cross BBB (has central effects). Long duration of action Direct muscarinic agonist (mainly on eye & secretion). Jaborandi (Pilocarpus pennatifolius)
Direct acting cholinergic agonists PILOCARPINE
Pilocarpine • Uses: • Xerostomia (dry mouth). • Drug of choice in emergency glaucoma applied as eye drops. • Adverse effects: • Profuse sweating • Salivation • Bronchoconstriction • Diarrhea • CNS effects
Aceclidinum • a synthetic preparation; • administered SC, IM, or topically(eye drops); not toxic; • does not penetrate CNS; • M-cholinomimetic; • used forthe treatment of atonia of the intestine and urinary bladder, as well as for glaucoma.
Mushroom poisoning • Miosis • Hyper salivation • Excessive sweating, lacrimation • Cold, wet skin • Bradycardia • Polyuria • Diarrhea • Convulsions Atropine
N-CHOLINOMIMETICS • They stimulate N-cholinoreceptors in zona carotis and initiate a reflexive increase • in the activity of the respiratory and vasomotor centers resulting in the shortstimulation of breathing and elevation of BP. • They also stimulate N-cholinoreceptors in the adrenal medulla, increase thesecretion of epinephrine, which causes vasoconstriction and the elevation of BP
NICOTINE • It is a tobacco alkaloid with a dose-dependent action on N-cholinoreceptors. • Effects of nicotine are manifested in tobacco smoking. • Nicotine causes dependencethat leads to abuse of tobacco and results in the development of cardiovascular andlungs pathology.
Physiological effects of nicotine at CNS NN receptors • • ↑Emesis (vomiting) due to actions on chemoreceptor trigger zone of medulla oblongata • • Dependence (i.e. makes it hard to quit smoking) • • Respiratory depression (only at very high doses) due to actions on medulla oblongata - also contribution from blockade of diaphragm and intercostal muscles • • Tremors + convulsion (only at very high doses)
Physiological effects of nicotine at peripheral NN receptors • Many Effects of Nicotine Involve Ganglia • • ↑GI motility (nausea, diarrhea, vomiting) – Stimulation of parasympathetic ganglia • • ↑Heart rate, ↑blood pressure – Stimulation of sympathetic ganglia innervating heart and blood vessels – Release of EPI from adrenal medulla – Stimulation of chemoreceptors → reflex ↑heart rate, vasoconstriction
Lobeline • is an alkaloid; is administered IV and acts during 3-5 min; • stimulates N-cholinoreceptors; • is used for emergency help in the respiratoryarrest, asphyxia, asphyxia of newborns; is used to treat tobacco abuse in the formof combined tablets • is not used for collapse due to its ability to provoke transitory a decrease in BP resulting from the stimulation of n.vagus center.
Cytitonum • the name of a cytizine solution; • administered IV, acts 3-5 min; • stimulates N-cholinoreceptors; reflexly stimulates respiration and increases BP; • used for emergency help in respiratory arrest and collapse; • an ingredient of combinedtablets against tobacco abuse.
Indirect acting cholinergic agonists Reversible Irreversible Edrophonium Neostigmine Physostigmine Rivastigmine Galantamine Echothiophate Organophosphates Arminum
Mechanism of action: Anticholinesterasesprevent hydrolysis of Ach by antagonizing cholinesterase thus increase Ach concentrations and actions at the cholinergic receptors(both nicotinic and muscarinic). Mechanism of action
Pharmacological effects of anticholinesterases • Muscarinic actions • Nicotinic actions • CNS actions: Excitation, convulsion, respiratory failure, coma only for lipid soluble anticholinesterases physostigmine & phosphate ester except Ecothiophate.
Reversible Physostigmine • Reversible anticholinesterase • Tertiary ammonium compound • Non polar (lipid soluble) • Good lipid solubility • Good oral absorption • Has muscarinic & nicotinic actions • cross BBB (has CNS effects) Calabar Bean
Reversible Physostigmine Indications 1. Atony of intestine 2. Atony of bladder 3. Glaucoma 4. Overdose of ATROPINE, ANTIPSYCOTICS, ANTIDEPRESSANTS Side effects • Convulsions • Bradycardia • Paralysis of skeletal muscle
Reversible Neostigmine • Quatenary nitrogen • Poor adsorbtion • Not penetrate BBB • Reversible anticholinesteras • Has muscarinic & nicotinic actions (prominent on GIT &urinary tract).
Reversible Neostigmine Side effects Indications • Salivation • Flushing • Decreased BP • Abdominal pain • Diarrhea • Bronchospasm • Paralyzes • Myastenia gravis • Antidote of neuro-muscular blocker TUBOCURARINE