Download
1 / 42
420 likes | 628 Views
CRANIAL NERVES V-VII. Cranial Nerve V: Trigeminal Nerve.

E N D
Cranial Nerve V: Trigeminal Nerve large sensory root, which carries sensation from the skin and mucosa of most of the head and face, and a smaller motor root, which innervates most of the chewing muscles (masseter, temporalis, pterygoids, mylohyoid), and the tensor tympani muscle of the middle ear.
The efferent fibers of the nerve (the minor portion) originate in the motor nucleus of V in the pons this cell group receives bilateral input from the corticobulbar tracts and reflex connections from the spinal tract of nerve V and controls the muscles involved in chewing.
The sensory root (the main portion of the nerve) arises from cells in the semilunar ganglion (also known as the Gasserian, or trigeminal, ganglion) in a pocket of dura (Meckel's cavity) lateral to the cavernous sinus. It passes posteriorly between the superior petrosal sinus in the tentorium and the skull base and enters the pons.
Fibers of the ophthalmic division enter the cranial cavity through the superior orbital fissure. Fibers of the maxillary division pass through the foramen rotundum. Sensory fibers of the mandibular division, joined by the motor fibers involved in mastication, course through the foramen ovale.
Trigeminal nerve fibers carrying light touch project to the main (principal) trigeminal nucleus After synapsing, this pathway passes from the nerve's main sensory nucleus via crossed fibers in the ventral trigeminothalamic tract and via uncrossed fibers in the dorsal trigeminothalamic tract to the ventral posteromedial (VPM) nuclei of the thalamus and higher centers.
Pain and temperature fibers in the trigeminal nerve enter the brain stem, turn caudally, and descend for a short distance within the spinal tract of V.
These fibers then synapse with secondary neurons in the spinal nucleus of V. From there, the pathway passes to the thalamus via the ventral trigeminothalamic tract. Proprioceptive fibers in the trigeminal nerve project to the mesencephalic trigeminal nucleus (mesencephalic nucleus of V), where their cell bodies are located. Collaterals project to the motor nucleus of V.
The reflex connections pass to the cerebellum and the motor nuclei of cranial nerves V, VII, and IX.
Corneal reflex The afferent axons for the reflex(in which corneal stimulation evokes a protective blink response) are carried in the ophthalmic branch of nerve V and synapse in the spinal tract and nucleus of V.
From there, impulses are relayed to the facial (VII) nuclei, where motor neurons that project to the orbicularisoculi muscles are activated. (The efferent limb of the corneal reflex is thus carried by nerve VII.)
The jaw jerk reflex monosynaptic (stretch) reflex for the masseter muscle. Rapid stretch of the muscle (elicited gently with a reflex hammer) evokes afferent impulses in Ia sensory axons in the mandibular division of nerve V, which send collaterals to the mesencephalic nucleus of V, which sends excitatory projections to the motor nucleus of V.
Both afferent and efferent limbs of the jaw jerk reflex thus run in nerve V.
Clinical Correlations Symptoms and signs of nerve V involvement include loss of sensation of one or more sensory modalities of the nerve impaired hearing from paralysis of the tensor tympani muscle paralysis of the muscles of mastication, with deviation of the mandible to the affected side
loss of reflexes (cornea, jaw jerk, sneeze) trismus (lockjaw) in some disorders, tonic spasm of the muscles of mastication.
Because the spinal tract of V is located near the lateral spinothalamic tract in the medulla and lower pons, laterally placed lesions at these levels produce a crossed picture of pain and temperature insensibility on the ipsilateral face and on the contralateral side of the body below the face.
This occurs, for example, in Wallenberg's syndrome, in which there is damage to the lateral medulla, usually because of occlusion of the posterior inferior cerebellar artery.
Trigeminal neuralgia characterized by attacks of severe pain in the distribution of one or more branches of the trigeminal nerve. Although the cause is not always clear, it is known that excruciating paroxysmal pain of short duration can be caused by pressure from a small vessel on the root entry zone of the nerve.
Trigeminal neuralgia is also seen in some patients with multiple sclerosis. Pain may follow even gentle stimulation of a trigger zone, a point on the lip, face, or tongue that is sensitive to cold or pressure. Involvement is usually unilateral.
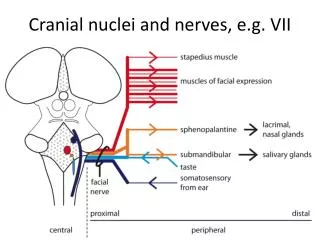
Cranial Nerve VII: Facial Nerve The facial nerve consists of the facial nerve proper and the nervusintermedius Both parts pass through the internal auditory meatus, where the geniculate ganglion for the taste component lies. The facial nerve proper contains axons that arise in the facial (VII) nucleus.
The nerve exits through the stylomastoid foramen; it innervates the muscles of facial expression, the platysma muscle, and the stapedius muscle in the inner ear.
The nervusintermedius sends parasympathetic preganglionic fibers to the pterygopalatine ganglion to innervate the lacrimalgland via the chorda tympani nerve to innervate the submandibular and sublingual salivary glands.
The visceral afferent component of the nervusintermedius, with cell bodies in the geniculate ganglion, carries taste sensation from the anterior two-thirds of the tongue via the chorda tympani to the solitary tract and nucleus. The somatic afferent fibers from the skin of the external ear are carried in the facial nerve to the brain stem. These fibers connect there to the trigeminal nuclei and are, in fact, part of the trigeminal sensory system.
The superior salivatory nucleus receives cortical impulses from the nucleus of the solitary tract Visceral efferent axons run from the superior salivatory nucleus via nerve VII to the pterygopalatine and submandibular ganglia. They synapse there with postganglionic parasympathetic neurons that innervate the submandibular and sublingual salivary glands.
The taste fibers run through the chorda tympani and nervusintermedius to the solitary nucleus, which is connected with the cerebral cortex through the medial lemnisci and the VPM nucleus of the thalamus and with the salivatory nucleus and motor nucleus of VII by reflex neurons.
The facial nucleus receives crossed and uncrossed fibers by way of the corticobulbar (corticonuclear) tract The facial muscles below the forehead receive contralateral cortical innervation (crossed corticobulbar fibers only). Therefore, a lesion rostral to the facial nucleus—a central facial lesion—results in paralysis of the contralateral facial muscles except the frontalis and orbicularisoculi muscles.
Clinical correlations This can occur, for example, as a result of a stroke which damages part of the motor cortex in one cerebral hemisphere. Because the frontalis and orbicularisoculi muscles receive bilateral cortical innervation, they are not paralyzed by lesions involving one motor cortex or its corticobulbar pathways
The complete destruction of the facial nucleus itself or its branchial efferent fibers (facial nerve proper) paralyzes all ipsilateral face muscles; this is equivalent to a peripheral facial lesion.
Peripheral facial paralysis (Bell's palsy) can occur as an idiopathic condition, but it is seen as a complication of diabetes and can occur as a result of tumors, sarcoidosis, AIDS, and Lyme disease When an attempt is made to close the eyelids, the eyeball on the affected side may turn upward (Bell's phenomenon
The symptoms and signs depend on the location of the lesion. A lesion in or outside the stylomastoid foramen results in a flaccid paralysis (lower-motor-neuron type) of all the muscles of facial expression in the affected side this can occur from a stab wound or from swelling of the parotid gland (eg, as seen in mumps).
A lesion in the facial canal involving the chorda tympani nerve results in reduced salivation and loss of taste sensation from the ipsilateral anterior two-thirds of the tongue. A lesion higher up in the canal can paralyze the stapedius muscle.
A lesion in the middle ear involves all components of nerve VII tumor in the internal auditory canal (e.g., a schwannoma) can cause dysfunction of nerves VII and VIII.