Download
1 / 25
280 likes | 791 Views
Case study Esophagus. Dr W.J. Conradie Department of D iagnostic Radiology March 2012. 93 year old Caucasian female. Housewife No previous major surgery Medical history: Hypertensive with mild CCF on medication. Irritable bowel syndrome Medication: Fosamax Disprin Adco Dol

E N D
Case studyEsophagus Dr W.J. Conradie Department of Diagnostic Radiology March 2012
93 year old Caucasian female • Housewife • No previous major surgery • Medical history: • Hypertensive with mild CCF on medication. • Irritable bowel syndrome • Medication: • Fosamax • Disprin • AdcoDol • Enalapril and Lasix • Family history: • Eldest son died of esophagealCa in 2007
2008: Presented with.. • Progressive dysphagia (solids/fluids) over couple of months. • Episodes of coughing while eating/drinking • Intermitted regurgitation of undigested food. • Feeling of “fullness” in neck • Weight loss ± 5kg
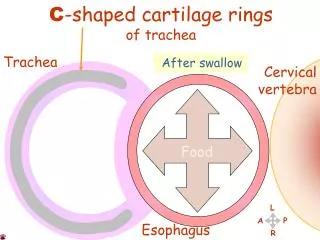
Clinically: • Large para-tracheal mass on the left extending into/through thoracic inlet • Moved with swallowing • No features of thyrotoxicosis • No cervical lymphadenopathy • Severe kypho-scoliosis
Special investigations: • CXR: • Degenerative spine • Clear lung fields • Bloods: • Normal • FBC, U&E, LFT • CRP and ESR • Thyroid functions • S-albumin
Special investigations:CT chest (19-06-2008) • Large irregular mass from left thyroid lobe • Extends deep into superior mediastinum • Cyst with calcifications inferiorly • Nodule in superior aspect of lobe with central breakdown • No mediastinallympnodes • Lung fields clear • Incidental: Aorta arch anomaly
Aorta arch anomaly: Main stem for right and left common carotid Left subclavian artery Aberrant right subclavian artery
Differential diagnosis for dysphagia Thyroid mass Zenker ‘s Diverticulem Aberant right subclavian artery (dysphagia lusoria) Achalasia
Zenker ‘s Diverticulem • Named after Friedrich Albert von Zenker who was a German pathologist (1825 – 1898) • Definition: • Mucosal outpouching of posterior hypopharyngeal wall. • Proximal to upper esophagealsphincter (Cricopharyngeal muscle) • Pathophysiology: • Pulsion-pseudodiverticulum with herniation of mucosa and submucosa through Killian’s dehiscence. • Focal weakness in cleavage plane between the fibers of inferior pharyngeal constrictor and cricopharyngeusmuscles. • Due to cricopharyngeal dysfunction luminal pressure
Zenker ‘s Diverticulem • Prevalence • <0.2% of general population • Elderly woman • >50% occur in 7th -8th decade • Clinically: • globus feeling • dysphagia • halitosis • regurgitation • Associated with: • Hiatus hernia • GER / Reflux oesophagitis • Achalasia • Complications • Aspiration • Perforation • Ulceration • Carcinoma • Differential diagnosis • Killian-Jamieson diverticulum (K-J) • Esophagealweb • Lateral pharyngeal pouch • Epidermolysisbullosadystrophica
Zenker ‘s DiverticulemImaging findings • General features: • Location: Killian’s dehiscence • Posterior above cricopharyngeus • C5-6 • Size: 0.5-8cm (average 2.5cm) • Best diagnostic clue: Barium filled sac! • Radiographic findings: CXR/CT: • Air-fluid level in superior mediastinum
Zenker ‘s DiverticulemImaging findings Barium swallow • AP: • Barium-filled sac below the level of hypopharynx • Lateral/oblique view: • Barium-filled sac posterior to cervical esophagus • Neck opening into posterior wall above cricopharyngeus m. • Prominent or thickened cricopharyngeal muscle • Luminal narrowing at upper pharyngoesophageal junction • ± Nasopharyngeal regurgitation
Dysphagia Lusoria • Dysphagia secondary to extrinsic esophagealcompression by an aberrant right subclavian artery • Described by Bayford in 1794 • lusoria- Greek phrase lususnaturae, meaning “ freak or zest of nature”, which refers to the freaky course of the artery (lusoria artery)
Dysphagia LusoriaAberrant Right Subclavian artery • Prevalence of 1.8% • 1/3 experience symptoms (90% = dysphagia) • Any age • Old age: atherosclerosis or aneurysmal dilatation of ARSA. • Associated: • Dyspnoea • Lower right arm BP/pulse volume • Diverticulum of Kommerell. • Management: • Conservative • Carotico-subclavianbypass
Achalasia • Definition: • Primary motility disorder of esophageal smooth muscle • Failure of LES to relax • “Failure to relax” • Sir Thomas Willis in 1672. • 1929: Hurt and Rake • Discovered failure of LES to relax. • Pathophysiology • Degeneration of Auerbach’s plexus • Primary(classic) - idiopathic (number decrease, CNX – nucleus or nerve) • Secondary - metastases, adenocarcinoma, vagotomy, scleroderma • Infectious - Chagas disease(trypanosomacrucineurotoxin destroys ganglia)
Achalasia • Prevalence • Primary: younger (20-50) • Secondary: older • Male=female • Clinically: • Dysphagia (solids and liquids) • Regurgitation • Weight loss in 90% • Diagnosis • Exclude malignancy • Exclude oesophageal spasm • Manometry • Complications: • Coughing • Aspiration • Pneumonia • Lung abscess • Esophagealcarcinoma (2-7%) • Management: • Aimed at improving esophageal emptying • Calcium channel blockers • Botulinumtoxin injection • Pneumatic dilatation • Heller myotomy
AchalasiaImaging findings • General findings • 2 criteria: • Absent primary/secondary peristalsis • LES fails to relax when swallowing • Tertiary waves • "Bird-beak" deformity • Dilated esophaguswith smooth, symmetric, tapered narrowing at GEJ
AchalasiaImaging findings CXR: • Mediastinal widening • Double contour • Anterior tracheal bowing • Air-fluid level in mediastinum • Small or absent gastric air bubble
AchalasiaImaging findings Barium meal Classic Achalasia • Dilated esophagus (>4cm) • Absent peristalsis • Distal segment • "Bird-beak" deformity • Hurst phenomenon: • transit when hydrostatic pressure of barium column is above tonic LES pressure • Narrowed segment: <3.5 cm in length Secondary Achalasia • Less dilated (<4 cm) • Decreased or absent peristalsis • Distal segment: • Eccentric, nodular, shoulder • smooth, symmetric, tapered • Narrowed segment: >3.5 cm
Achalasia Differential diagnosis • Scleroderma • Esophageal carcinoma • Gastric carcinoma • Esophagitis with stricture • Diffuse esophageal spasm
Back to grandma.. • Cause for dysphagia: Thyroid mass • Surgicaly removed 16-07-2008 • Histology: Benign, Non toxic Nodular goitre • Outcome (2012): • Improved but still suffers from dysphagia!! • Zenker’sdivertikulem? • ARSA? • THANK YOU
REFERENCES • Weissleder, Wittenberg, Harisinghani, Chen. Primer of Diagnostic Imaging. Fifth edition. 2011. • Federle, Jeffrey, Desser, Anne, Eraso. Diagnostic Imaging of the Abdomen. First edition. 2004. • (PPP) ZENKER’S DIVERTICULUM. N. D’Souza,Underbrink. 2010 • J. Dandelooy, J.P.M. Coveliers, P.E.Y. Van Schil, S.Anguille. Dysphagia lusoria. CMAJ • October 13, 2009 • 181(8) • P.D. Kent, T.H. Poterucha. Aberrant Right SubclavianArtery and Dysphagia Lusoria. N Engl J Med, Vol. 346, No. 21 May 23, 2002