Download

1 / 52
520 likes | 587 Views
Quality “Start Up” Measures and Instruments. R. Sean Morrison, MD Hermann Merkin Professor of Palliative Care Professor, Geriatrics and Medicine Vice-Chair for Research Department of Geriatrics & Adult Development Mount Sinai School of Medicine New York, NY. What is Palliative Care?.

E N D
Quality “Start Up” Measures and Instruments R. Sean Morrison, MD Hermann Merkin Professor of Palliative Care Professor, Geriatrics and Medicine Vice-Chair for Research Department of Geriatrics & Adult Development Mount Sinai School of Medicine New York, NY
The Rationale For Data Collection The Process of Data Collection Data Storage Data Presentation
Why Collect Data? • Research • Programmatic development • Needs assessment • Making the case • Program maintenance • Continued justification • Expansion • Clinical assessment
What Are The Variables? • Who are your patients? • What do they experience • What happens to them? • What do you do for them? • What do they cost? In other words…
Who are your patients? • Patient demographics and characteristics • Age • Sex • Diagnoses • Functional status • Next of kin (contact) • Referring physician • Advance directive status at time of consult • Presence and timing of DNR orders • Pain and other symptoms • Outcomes • In-hospital death rate, ICU death rate, length of stay
What happens to them? • Pain and other symptoms • Outcomes • In-hospital death rate • ICU death rate • Length of stay (hospital and ICU)
What do you do for them? • Impact of palliative care • Hospital discharge • Transfer out of ICU • Advance care planning/DNR discussions • Palliative care interventions • Family satisfaction
What do they cost? • Financial Outcomes • Length of stay • ICU length of stay • Length of stay after palliative care consultation • Costs • Total costs, direct costs, pharmacy costs, ancillary charges
What Are The Data Sources? • Patients • Proxies • Family members, friends, health care professionals • Medical record review • Hospital databases
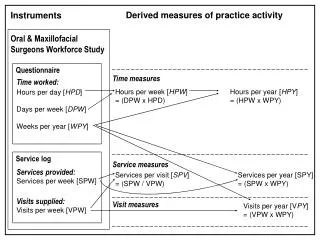
Reliable Valid Gold standard for pain; non-pain symptoms; psychological, spiritual, and social well being; quality of life Time intensive Labor intensive Patients are often too sick to participate Retrospective interviews are often impossible Patient Interviews: The Pros and the Cons
What Do You Need to Ask/Gather From Patients? • Demographic Information • Contact information, name/telephone number of proxy respondent • Demographics? • Race, religion • Functional status • Karnofsky/ECOG performance score, ADLs, IADLs • Advance directive status • Health care proxy, living will, DNR, verbal directives • Pain and symptom assessment
Available and accessible Retrospective interviews are possible Reasonable measure of quality issues Family experience Proxy experience Patient experience Validity of data dependent on proxy’s communication and connection with patient Proxy Interviews: The Pros and the Cons
What Do You Need to Ask/Gather From Proxies? • “Satisfaction” data • Process data • Caregiver burden • Identification of quality measures for your program • Processes of care • Outcomes
Easily accessible Relatively time efficient means of gathering data “If it’s not recorded, it didn’t happen” Limited to what is recorded Important information is sometimes not recorded Validity can be suspect Requires sophisticated abstractor Labor intensive Medical Record Review: The Pros and the Cons
What Do You Need to Gather From The Medical Record? • Advance directive documentation • Living will, health care proxy, presence and timing of DNR orders • Site of hospital discharge, referral to hospice • Diagnoses and comorbid illness • Pharmacy data • Palliative care “interventions”
Accessible Population data No data entry required Relatively easy to manipulate Limited to what is abstracted and stored Variable reliability The route to the data is tortuous Who has the data? Can you access it? What does a data request require? What form do you need it in? Can you manipulate it? Databases are intimidating Hospital Databases: The Pros and the Cons
What Do You Need to Gather From Databases? • Patient characteristics and demographics • Age, sex, insurance status, DRG, diagnostic and procedure codes • Length of stay (ICU and hospital) • Costs (total, direct, ancillary, pharmacy) • Pharmacy data (if available) • Analgesics, Antiemetics, Laxatives, Antidepressants, Anxielytics
Choosing and Designing Your Instruments: Measurement 101 • Patient interview forms • Demographic and contact information • Pain and symptom assessment • Chart abstraction instrument • Team audit instrument • Post-discharge/death patient family satisfaction
Keys to Instrument Development • What are the key elements that you can’t live without? • Everything gets a code • 7 – refused, 8 – not applicable, 9 – missing • Circling is easier and faster than writing • Avoid text wherever possible – use numbers • Pilot your instrument • Collect your programmatic data as part of your clinical assessments • Handheld computers
Patient Interview Forms • Initial consultation form • Appendix 1 • Pain and symptom assessment • Appendix 2a – ESAS • Appendix 2b – PCLC instrument • Appendix 2c – Condensed MSAS
Patient Interview/Chart Abstraction Instrument • Appendix 2b • PCLC clinical instrument
Team Audit Instrument • Appendix 3
Patient and Family Satisfaction • After Death Bereaved Family Interview – Appendix 4 • Hospital, hospice, and nursing home versions • FAMCARE – Appendix 5 • Palliative Care Outcome Scale (POS) – Appendix 6
Setting Up Your Database • Necessary • “Database” options: • Spread sheets (Excel, Lotus, Quattro) • Patients are rows • Variables are columns • Statistical packages (SAS, Stata, SPSS) • Databases (MS Access) • Simple forms that mimic your paper forms • Data stored in corresponding tables
Sources For Database Help • Hospital Information Technology • Local community colleges, graduate psychology/sociology programs • Billing/finance administrator • Reference Manuals
Programmatic Development • Your message • Your hospital needs a palliative care program • The financial incentives favor the development of a palliative care program • Your data • Your patient population • Their symptom burden • Their costs
Programmatic Development • Your data collection • Database review of all deaths in the last calendar year • Mean age, sex, insurance, DRG, ICD-9 code(s) • Convert DRG’s, ICD-9 codes to common diagnoses • Length of stay, Number of ICU days • 25 consecutive cancer admissions • Symptom assessment • Analgesic prescribing • Costs and Estimates of Savings
Demographics of Patients Who Die At Mount Sinai Hospital Source: Billing Database
Symptom Burden of 542 Cancer Patients Hospitalized Mount Sinai • 25% reported moderate-severe pain on admission • 28% continued to experience moderate-severe pain 3 days later • 20% reported having moderate to severe pain for over half of their admission • 1/3 of patients with moderate-severe pain received only “prn” or as needed analgesics • 16% were discharged from hospital with moderate to severe pain • 14% were discharged from hospital with severe nausea • 46% were discharged from hospital with severe constipation
Suggested baseline measures (financial/utilization) • % of patients who die in the ICU • LOS in ICU for target DRGs • Cost per day & per case by DRG • “Diversions” • Discharge sites • Number & costs of outliers for DRGs
Programmatic Maintenance • Your message • Your program improves clinical care • Patient/family satisfaction is high • Your program is fiscally responsible • Your data • Description of your patients • Impact of your program on pain and other symptoms • Fiscal parameters • Length of stay, transfers from ICU to palliative care, discharge to hospice • Pharmacy data
Programmatic Maintenance • Your data collection • Patient descriptors from your interview form, medical record abstraction form, hospital database • Vignettes • Pain and symptom data from your clinical assessments • Palliative care interventions from your clinical team audit • Patient/Family Satisfaction • Length of stay data from your medical records/hospital billing system • Cost data
Palliative Care Program Patient Characteristics (1997-2000) • Median Age 71.4 (range 18 to 104) • 54% Women • 48% White, 23% African American, 23% Latino, 5% Other • 63% Medicare • 25% of all hospital deaths • Performance status at time of consult: • Moribund 17% • Very sick requiring active supportive treatment 32% • Severely disabled 26% • Disabled requiring assistance 14% • Normal activity but requiring frequent medical care 11% Source: palliative care database
Improvement in Symptoms for Patients Followed by the Palliative Care Service Pain Nausea Severe Severe Mod. Mod. Mild Mild None None Shortness of Breath Anxiety Severe Severe Mod. Mod. Mild Mild None None
Percent of Palliative Care Families Satisfied or Very Satisfied Following Their Loved Ones Death With: • Control of pain - 95% • Control of non-pain symptoms - 92% • Support of patient’s quality of life - 89% • Support for family stress/anxiety - 84% • Manner in which you were told of patient’s terminal illness - 88% • Overall care provided by palliative care program- 95% Source: Post-Discharge/Death Family Satisfaction Interviews
Palliative Care Recommendations Forego Life Sustaining Treatment Source: Team Audit
LOS in Days in 2004 For Patients With LOS>10 days (Mean time to PC referral = 9.8 days)
Impact of Palliative Care on Reduction of ICU days • 61% of patients who die spend time in an ICU. • Mean ICU LOS for patients who die and who spend time in an ICU = 14 days • Palliative care reduces ICU LOS by 10 days for those with ICU LOS >14 days and by 16 days by those with ICU LOS > 42 days by transferring patients to more appropriate care settings Source: Hospital Financial Database and Palliative Care Database
Mean Direct Costs Per Day for The 35 Days Prior to Death Median Day of First Palliative Care Consult
Mean Direct Hospital Costs/Day P<.001 for all comparisons in multi-variate analyses
Mean Direct Hospital Costs/Day For Palliative Care and Usual Care Patients Admitted to an ICU* P<.001 P<.001 P=.001 P=.08 *198 palliative care patients in ICU at time of consult (54%) 573 Usual care patients admitted to ICU (55%)
Clinical Assessment • Your message • What do I need to improve patient care? • Your data • Pain and symptom assessment • Advance directive completion rates • Patient satisfaction • Medication prescribing
Clinical Assessment • Your data collection • Serial pain and symptom assessments as part of your clinical care • Documentation of advance care planning discussions • Clinical team audit after completion of consultation, discharge of patient, or death • Post death interviews with every nth patient’s family
Clinical Assessment: Edmonton Symptom Assessment Scale Bruera & Macdonald. In Higginson (ed). Clinical Audit in Palliative Care, 1993
Summary and Discussion • Data are essential for programmatic justification, maintenance, clinical care, and quality • Target different sources for data collection • Patient, proxy, medical record, databases • Select sources based upon institutional resources • Use standardized instruments • Electronically store your data • Use data to support and convey your message